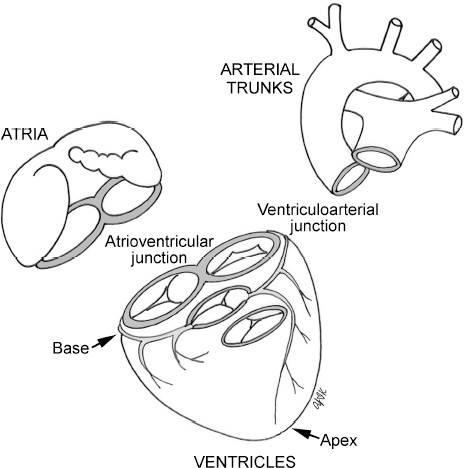
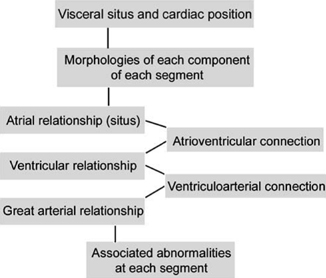
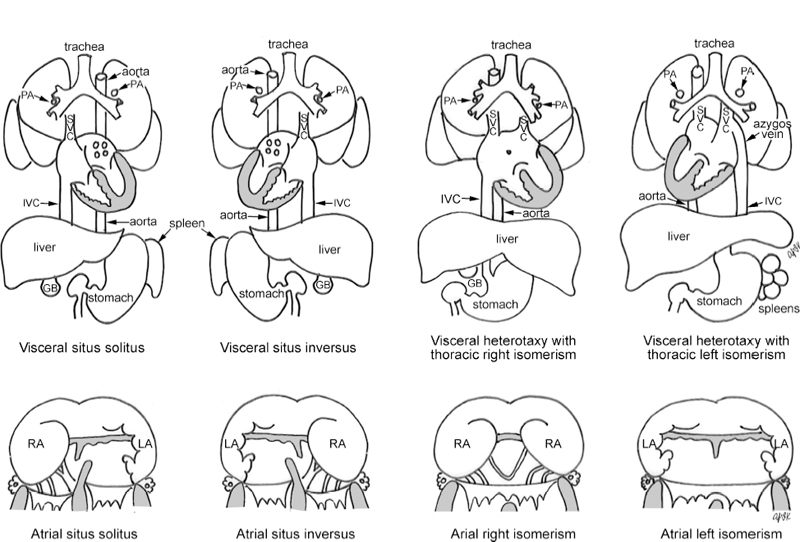
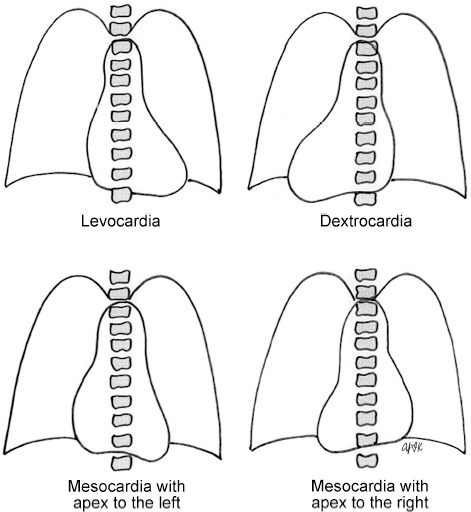
2 Sequential Segmental Approach to Congenital Heart Disease Morphologically, malformations affecting the heart can be categorized into two broad categories. The first category is the malformations affecting the heart in which the cardiac chambers and the great arteries are normally related and connected. Typical examples are septal defects and valvular stenosis. The second category includes more complex malformations that are characterized by an abnormal relationship between the components of a segment or segments and abnormal connections between cardiac segments. Examples include various forms of so-called single ventricles or univentricular hearts, complete and corrected transposition of the great arteries, and double-outlet ventricles. These complex malformations require a systematic analysis in a step-by-step fashion that is called the sequential segmental approach.1–6 The concept of sequential segmental approach was first introduced by Van Praagh et al in 1964.7 Since then, there have been discussions and debates regarding the system of segmental analysis and its terminology. The most intense and serious debates have been between Richard Van Praagh of Boston, Massachusetts, and Robert H. Anderson of London, UK. Unfortunately, the debates have polarized the pediatric cardiology group into two schools, Van Praaghnians and Andersonians. On reading the published book chapters and articles regarding this important subject, one may be overwhelmed by the semantic controversies and debates. In this chapter, we will introduce the compromised system and terms that we find most useful in day-to-day clinical practice without discussion of the scholastic origins of the terms. As discussed in Chapter 1, the heart consists of three morphologically and functionally distinct segments: the atria, the ventricles, and the arterial trunks (Fig. 2.1). They are joined together by two connecting units, the atrioventricular junction and the ventriculoarterial junction, both of which are usually guarded by the valves. Each component of each segment of the heart is characterized by its own morphologic characteristics. The components of each segment can be related in various ways, and the components of a segment can be connected to the components of the next segment in various ways. Therefore, there are three facets in the make-up of the heart: the morphologies, the connections, and the relations.6 Sequential segmental analysis is the systematic approach to the diagnosis of congenital heart disease in which the three facets of the make-up in the heart are analyzed in a segment-by-segment fashion. The major steps of sequential segmental approach include (Fig. 2.2) Fig. 2.1 Basic cardiac segments and intervening junctions. Fig. 2.2 Steps of the sequential segmental approach. Congenital heart disease is common and usually complex when the visceral situs is abnormal or the heart is abnormally positioned. As will be discussed later in this chapter, the visceral situs is highly predictive of the atrial situs, which is called the visceroatrial concordance rule. Therefore, the visceral situs should be determined as the first step of a segmental approach. Fig. 2.3 Types of visceral and atrial situs. PA, pulmonary artery; SVC, superior vena cava; IVC, inferior vena cava; GB, gallbladder; RA, right atrium; LA, left atrium. The visceral situs is classified into the situs solitus, situs inversus, and heterotaxy. In situs solitus, the larger lobe of the liver is seen on the right, and the stomach and spleen are seen on the left (Fig. 2.3). The abdominal aorta is located posteriorly at the left anterior aspect of the spine, and the inferior vena cava is located more anteriorly on the right as it connects to the right atrium. In situs inversus, this right-left relationship is reversed. Rarely, the arrangement of the abdominal organs does not conform to the orderly and lateralized pattern of the situs solitus or the situs inversus. This condition is called visceral heterotaxy.3,4 Usually visceral heterotaxy is associated with either polysplenia or asplenia. It is important, therefore, to evaluate the splenic status by scrutinizing the perigastric area when the abdominal situs is neither solitus nor inversus. In polysplenia, multiple spleens of similar size are seen behind the stomach as they are aggregated on both sides of the mesogastrium. Occasionally, multiple spleens may be fused to form a single but multilobulated mass. Polysplenia is commonly associated with interruption of the suprarenal segment of the inferior vena cava with continuation through the azygos or hemiazygos venous system. Although it can also occur with any other body situs, interruption is highly suggestive of polysplenia.8,9 In most cases of asplenia, the abdominal aorta and inferior vena cava are juxtaposed on the same side of the spine.8–10 In the thorax, visceral heterotaxy is characterized by a symmetric lobation of the lungs and a symmetric branching pattern of the bronchi and pulmonary arteries. Visceral heterotaxy with asplenia is typically associated with a right isomeric arrangement of the lungs, bronchi, and pulmonary arteries, whereas visceral heterotaxy with polysplenia is usually associated with a left isomeric arrangement. The cardiac positions are classified into levocardia, dextrocardia, and mesocardia according to where the main part of the heart is located relative to the midline (Fig. 2.4). With rare exceptions, the main part of the heart is positioned on the side where the cardiac apex is located. In mesocardia, the cardiac apex may point to the right, left, or midline. These terms should not be used for those conditions where the heart is displaced to either side secondary to a noncardiac pathology such as hypoplasia or hyperinflation of a lung. Complex terms, such as dextroversion, levoversion, and dextroposition should be abandoned. Fig. 2.4 Cardiac positions. After determination of the visceral situs and cardiac position, the cardiac chambers and great arteries are identified according to the morphologic characteristics. In this regard, one should be aware that the adjectives “right” and “left” for the cardiac chambers are not to describe the sidedness within the body, but to describe the morphology of the atria and ventricles. Therefore, the atrium that is located on the right, but shows the morphologic characters of the normal left atrium should be called “the right-sided (morphologically) left atrium.” The morphologic criteria for atrial, ventricular, and great arterial identification are discussed in Chapter 1 and summarized in Tables 2.1, 2.2, 2.3. The atrial situs means how the atria are related to each other relative to the midline. It is categorized into the situs solitus, situs inversus, right isomerism, and left isomerism (Fig. 2.3). As discussed, determination of the atrial situs is based on the morphology of the atrial appendages and the extent of the pectinate muscles relative to the atrioventricular junction.11 Although these criteria are easy to apply at pathologic examination, they are often inapplicable during diagnostic imaging of living individuals. It is well known, however, that the atrial situs is harmonious with the visceral situs in the majority of cases. Therefore, the atrial situs can be accurately predicted by analyzing the bronchial branching pattern and splenic situs. Lastly, it should be emphasized that an atrioventricular block in the presence of structural heart disease is highly suggestive of left atrial isomerism.12
 Basic Cardiac Segments and Steps of Sequential Segmental Analysis
Basic Cardiac Segments and Steps of Sequential Segmental Analysis
 Determination of the Visceral Situs and Cardiac Position
Determination of the Visceral Situs and Cardiac Position
 Morphologic Identification of the Cardiac Chambers and Great Arteries
Morphologic Identification of the Cardiac Chambers and Great Arteries
 Analysis of the Segmental Connections and Relations
Analysis of the Segmental Connections and Relations
Determination of the Atrial Situs
| Right Atrium | Left Atrium | |
| Sulcus and crista terminalis | Yes |





