More common in SB (up to 30%) and multivisceral Tx than most other solid organ transplant recipients
More common within SB allografts than in host organs
• Rejection and graft-vs.-host disease
Both common, cannot be distinguished on imaging
• Dilation of SB lumen
May result from dysmotility, adhesion, ischemia, or rejection
• Imaging protocols: Multiplanar CT, ± CT angiography, displays most important anatomical and pathophysiological information pertinent to small bowel Tx
• Upper GI series to evaluate motility and status of proximal bowel anastomosis
• Worse than for solid organ transplant recipients
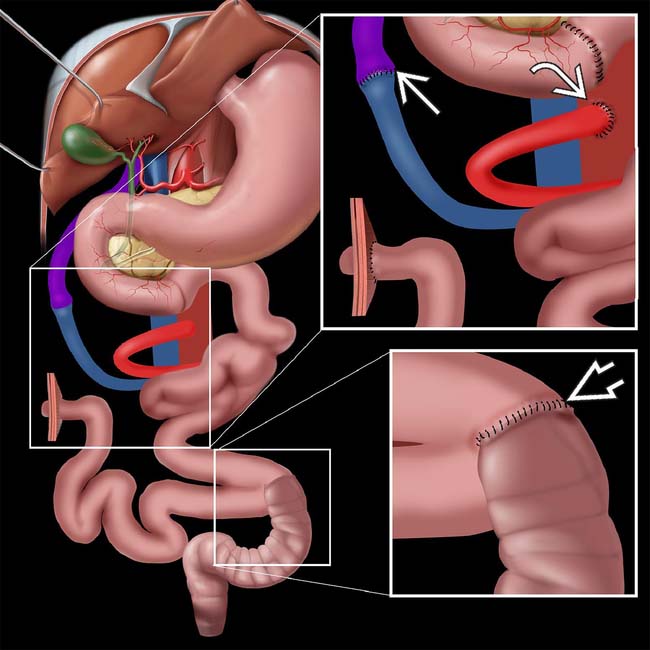
Graphic demonstrates some of the altered anatomy in a small bowel transplantation (SB Tx) procedure. The small bowel allograft is usually anastomosed proximally to the distal duodenum or proximal jejunum of the recipient, and distally to the sigmoid , with a temporary “chimney” ileostomy in the right lower quadrant. This ostomy allows convenient access to the allograft in the perioperative period for endoscopic visualization and biopsy procedures, and may be permanent. The donor superior mesenteric vein (SMV) is anastomosed to the host SMV or portal vein . The donor SMA is anastomosed to the host aorta .
TERMINOLOGY
Abbreviations
• Small bowel transplantation (SB Tx)
Indications for Small Bowel Transplantation
• Primarily for “short gut syndrome,” but also other causes of intestinal failure
Small bowel length or function insufficient to provide adequate nutrition
– Result of various etiologies
Superior mesenteric arterial (SMA) or venous (SMV) thrombosis with bowel ischemia, Crohn disease, midgut volvulus, familial polyposis/Gardner (especially with mesenteric desmoids)
– Much less commonly due to intestinal pseudoobstruction or other functional deficiency of small bowel
Patients can be maintained on total parenteral nutrition (TPN) indefinitely, except for complications
– Lack of central venous access to administer TPN, TPN catheter-related sepsis, and TPN-induced cholestatic liver disease
• Indications for multivisceral transplantation (liver, ± pancreas, ± part of stomach)
Advanced liver disease due to TPN or unrelated cause (e.g., chronic hepatitis)



 More common in SB (up to 30%) and multivisceral Tx than most other solid organ transplant recipients
More common in SB (up to 30%) and multivisceral Tx than most other solid organ transplant recipients




 , with a temporary “chimney” ileostomy in the right lower quadrant. This ostomy allows convenient access to the allograft in the perioperative period for endoscopic visualization and biopsy procedures, and may be permanent. The donor superior mesenteric vein (SMV) is anastomosed to the host SMV or portal vein
, with a temporary “chimney” ileostomy in the right lower quadrant. This ostomy allows convenient access to the allograft in the perioperative period for endoscopic visualization and biopsy procedures, and may be permanent. The donor superior mesenteric vein (SMV) is anastomosed to the host SMV or portal vein  . The donor SMA is anastomosed to the host aorta
. The donor SMA is anastomosed to the host aorta  .
. Small bowel length or function insufficient to provide adequate nutrition
Small bowel length or function insufficient to provide adequate nutrition








 Stomach (if included, usually in multivisceral transplants)
Stomach (if included, usually in multivisceral transplants) Intestine
Intestine Vasculature
Vasculature












