The spinal cord is an integral part of the neural axis or central nervous system. Disease entities in the brain or spinal cord may have a direct or indirect influence on each other. Imaging of the pediatric spine differs from that in adults in terms of relevant anatomy and associated pathology. An accurate imaging evaluation requires familiarity with the wide differential diagnosis of pediatric spinal disease. Spinal disease in children includes common processes, such as infection, trauma, and neoplasia. Developmental abnormalities of the spine require a thorough understanding of spinal embryology. A complete evaluation of the spine should include the bones of the spinal column, spinal canal, covering meningeal layers, and the spinal cord itself. The imaging technique of choice may differ depending on the age of the patient and the entity being evaluated. In this chapter, we will discuss the imaging techniques, embryology and development, and radiologic findings of developmental abnormalities and various spinal diseases in children.
Imaging Techniques
Plain Films
Conventional radiography (CR) is the initial modality of choice for evaluation of the osseous structures of the spine after trauma, scoliosis, atlantoaxial (AA) instability, and formation/segmental anomalies. Frontal and lateral projections of the spine are typically obtained. However, depending on the indication, further views or follow-up imaging may be required. For instance, scoliosis often requires serial CR examinations to monitor evolution of the curvature. The scoliosis curvature may be influenced by patient posture—that is, sitting, standing, lying supine or bending. CR is often the initial modality for the evaluation of back pain in children and may be used to screen for congenital, traumatic, neoplastic and infectious causes of pain. Back pain with scoliosis is considered a red flag for the presence of underlying spinal pathology in children. Hence back pain with scoliosis should be investigated with a thorough clinical history, physical examination, laboratory tests, and neuroimaging including magnetic resonance imaging (MRI). Increasingly, concern over radiation exposure in children has resulted in the substitution of MRI for CR and computed tomography (CT) for the evaluation of scoliosis, formation/ segmentation anomalies and craniocervical junction (CCJ) instability. CR, however, remains an important imaging tool of the spine but must be used according to the “as low as reasonably achievable” (ALARA) principle.
Ultrasound
Ultrasound is a portable, bed-side, readily available, and radiation-free technique that is extremely helpful in the evaluation of neonates and young infants. The most common indication in the neonate is closed spinal dysraphism, which includes lesions such as dorsal dermal sinus tracts. Images are obtained in the longitudinal and transverse planes using a linear 5- to 12-MHz transducer with the patient lying prone. Dynamic real-time images can be acquired to assess movement of the lumbosacral nerve roots if there is a question of spinal cord tethering. Counting down from the 12th rib and counting up from the sacral elements will determine the vertebral level. If the vertebral level is unclear, CR may be helpful for correlation with markers. Color or power Doppler ultrasound may be used as an adjunct to characterize soft tissue masses on the skin or within the spinal canal.
Magnetic Resonance Imaging
MRI represents the modality of choice for imaging of the spine and the spinal canal contents. The strengths of conventional MRI include its unique contrast resolution, multiplanar capability, and high-resolution isotropic three-dimensional (3D) acquisitions. Diffusion tensor imaging is an advanced MRI technique that allows for studying the white matter tracts in vivo. Diffusion tensor imaging may be used when there is a suspicion of spinal cord ischemia or infarction. In addition, functional imaging, for example, of cerebrospinal fluid (CSF) flow can be measured.
The conventional MRI protocol includes sagittal T1- and T2-weighted images plus axial T2-weighted images of the entire spine (as one or more series) from the posterior fossa through the coccyx. The sequences can be performed with and without fat saturation. Fat saturation is helpful to confirm bone marrow edema or for assessment of intraspinal fatty lesions (eg, lipoma). In addition, axial T1-weighted images may be added to evaluate for filar thickening, extent of a dermal sinus, and a tethering mass (eg, lipoma) or subacute hemorrhage. Coronal T2-weighted images assist in evaluating for spinal column anomalies (eg, hemivertebra in congenital scoliosis), split-cord malformations (eg, diastematomyelia), and renal anomalies. Sagittal short tau inversion recovery (STIR) images are helpful in the evaluation of ligamentous injury after trauma and the presence of marrow edema in infectious processes. T1-weighted acquisitions after intravenous gadolinium administration, both with and without fat saturation, in sagittal and axial planes, enhance the ability of MRI to evaluate inflammation and tumor, whether intramedullary, intradural, or extradural.
MRI is the imaging modality of choice for evaluating the bone marrow, intervertebral disks, and extradural soft tissues. Bone marrow signal intensity in children is age dependent due to its varying content of hematopoietic and fatty marrow. T1 signal intensity of hematopoietic marrow is equal to or slightly higher than muscle but less than fat. Diffuse marrow involvement in systemic disease (leukemia) with marrow replacement or localized bone marrow edema (traumatic/inflammatory) is best evaluated with T1-weighted images without fat suppression and T2-weighted images with fat suppression. For evaluation of extradural traumatic, inflammatory, or neoplastic processes (eg, ligamentous injury, disk herniation, osteomyelitis, sarcoma), sagittal T1-weighted images are performed, followed by sagittal fat-suppression T2-weighted or STIR images. Additional gadolinium-enhanced sagittal and axial fat-suppression T1-weighted images are necessary for evaluating neoplastic and inflammatory processes, as well as for assessing recurrent disk protrusion (nonenhancing) from scar (enhancing) after disk surgery. These techniques allow for the complete assessment of marrow, bony, and paraspinal soft tissue involvement and extent, as well as for spinal cord, cauda equina, or nerve root compression. Gadolinium enhancement is also necessary in the assessment of intramedullary tumors (eg, astrocytoma, ependymoma, and ganglioglioma) and intradural tumors (eg, neurofibroma and schwannoma), and for neoplastic leptomeningeal seeding (eg, medulloblastoma and germ cell tumors).
Sagittal and axial T2-weighted MRI may also be done in flexion and extension (with patient cooperation or physician supervision) to assess craniocervical instability or fixation (eg, craniocervical anomalies). Sagittal T2-weighted or STIR imaging, along with axial T2-weighted imaging and postcontrast T1-weighted imaging, is helpful to evaluate for intramedullary inflammation or degeneration, including the assessment of spinal cord atrophy. A combination of sagittal and coronal T1- and T2-weighted imaging plus axial T2-weighted imaging is performed for screening of patients with suspected spinal vascular malformation.
Additional pulse sequences may be helpful in certain circumstances. For example, hemorrhage is best demonstrated using gradient recalled echo (GRE) techniques (eg, MEDIC—a fast T2-weighted two-dimensional spoiled GRE multiecho sequence), which can be positive as early as 3 hours after trauma. High-resolution sequences (eg, a heavily T2-weighted high-resolution isotropic 3D-constructive interference in steady state [CISS] or 3D-T1 magnetization-prepared rapid gradient-echo (MPRAGE), a fast GRE sequence with fat saturation, with multiplanar reconstruction (MPR) may be helpful in the evaluation of sinus tracts, CSF leaks, or pseudomeningocele. Functional assessment of CSF movement can be achieved by using “velocity-encoded imaging” which may be useful in planning posterior fossa decompression in Chiari I malformation.
Computed Tomography
Computed tomography (CT) imaging of the spine is typically performed without the administration of intravenous contrast. Axial images are obtained followed by coronal and sagittal MPR in bone and soft tissue kernels. CT is replacing CR and becoming the standard for the emergency evaluation of spine trauma. However, due to the relatively greater radiation exposure with CT compared to CR, CT should be restricted for use to areas in question on CR or to assess for additional injury when there is evidence of osseous trauma or ligamentous injury on CR. CT continues to be the choice for assessment of localized bony abnormalities, particularly when the level is precisely defined clinically or by plain film, single-photon emission computed tomography (SPECT), or MRI (eg, diastematomyelia, spondylolysis, spinal stenosis, spondylitis, bone tumor—ie, osteoid osteoma or aneurysmal bone cyst). Axial sections with two-dimensional reformatting (coronal, sagittal, or oblique) and/or 3D reconstructions are often important in the preoperative evaluation of spine trauma, craniocervical anomalies, and congenital scoliosis, as well as for the postoperative assessment of instrumentation and fusion. CT may also be obtained (with patient cooperation or physician supervision) with the spine in flexion and extension or with right and left head turning, to evaluate for translational craniocervical instability or rotatory atlanto-axial (AA) instability or fixation, respectively. CT myelography is rarely needed except when MRI is contraindicated or spinal instrumentation does not allow adequate MRI quality. It may also assist in the more precise delineation of nerve root or other intradural lesions (eg, cysts). A water-soluble, low-osmolar, nonionic contrast material specifically approved for myelography is used because of its low toxicity and infrequent side effects. These techniques are best used in a limited and selective manner and using ALARA guidelines to minimize radiation exposure.
Radionuclide Imaging
Radionuclide imaging plays an important role in the evaluation of children with suspected infection. In vitro radiolabeling of leukocytes with 111 In-oxyquinoline or 99m Tc-HMPAO (hexamethylpropyleneamine oxime) may be helpful to localize bacterial infection. Bone scintigraphy with 99m Tc-labeled diphosphonates ( 99m Tc-methyl diphosphonate) and single-photon emission CT (SPECT) is frequently helpful for evaluating children with lesions of the spinal column (eg, osteoid osteoma and metastases). Fluorine 18-fluorodeoxyglucose positron emission tomography (PET) is used for infection and tumor imaging. PET (including PET-CT) is also used in the assessment of treatment response or tumor progression in childhood neoplasia.
Embryology and Normal Development
The normal development of the spinal canal and its contents involves four principal processes: (1) gastrulation with development of the notochord, (2) primary neurulation with ganglion development, (3) segmentation with appearance of the somites, and (4) secondary neurulation (caudal cell mass).
The first stage of gastrulation occurs during the second or third week of embryonic development and involves conversion of the embryonic disk from a bilaminar disk (ectoderm and endoderm) to a trilaminar disk composed of ectoderm, mesoderm, and endoderm. Ectodermal cells glide between the ectoderm and endoderm; most of the ectodermal cells migrate laterally to form the mesoderm, and those that remain in the midline migrate along the craniocaudal axis of the primitive streak to form the notochordal process. At 20 days of life, resorption of the floor of the notochordal process results in the definitive notochord. The definitive notochord defines the primitive axis and skeleton of the embryo and is eventually replaced by the vertebral column.
The second stage of primary neurulation occurs during the third or fourth week of embryonic development. The notochord induces the transformation of the overlying ectoderm into neuroectoderm with formation of the neural plate signaling the onset of primary neurulation. The neural plate transforms to a neural groove, bends, and folds to form the neural tube, which then closes. During the closure of the neural tube, the overlying neuroectoderm progressively detaches from the adjacent surface ectoderm. This process is known as disjunction. Surface ectoderm closes and covers the neural tube. Simultaneously, cells at the border of the neuroectoderm and ectoderm detach and form the neural crests. The neural crests subsequently fragment and give rise to the primordia of the ganglia, which again give rise to the sensory nerves. The corresponding level of the neural tube and later the spinal cord furnishes the motor nerves. Primary neurulation is responsible for the development of the brain and upper 90% of the spinal cord.
The third stage of embryonic development involves forming a somite plate on each side of the neural tube. At the end of the fifth week of gestation, 42 pairs of somites are formed. The somites further differentiate into sclerotomes, dermatomes, and myotomes.
The fourth or final stage is secondary neurulation, which occurs between the fifth and sixth week of embryonic life during which the lower 10% of the spinal cord and filum terminale develop. A portion of the neural tube also known as the secondary neural tube develops from the caudal cell mass to the posterior neuropore. The caudal cell mass is derived from the caudal end of the primitive streak. The caudal cell mass is initially solid but subsequently undergoes a process of cavitation and canalization, eventually forming the tip of the conus medullaris and filum terminale by a process called retrogressive differentiation.
Developmental Abnormalities
A malformation is defined as a congenital morphologic anomaly of a single organ or body part caused by an alteration of the primary developmental program. Based on the normal processes of development of the spinal canal and its contents, malformations can be classified as: (1) disorders of primary neurulation, (2) disorders of secondary neurulation, or (3) anomalies of notochordal development.
Disorders of Primary Neurulation
From a clinical and embryologic perspective, disorders of primary neurulation can be divided into (1) open spinal dysraphism, (2) closed spinal dysraphism, and (3) dorsal dermal sinus. In an open spinal dysraphism, there is a defect in the overlying skin, and the neural tissue is exposed to the environment. In closed spinal dysraphism, the malformed neural tube is covered by mesodermal (subcutaneous fat) and ectodermal (skin) elements.
Open (Non–Skin–Covered) Spinal Dysraphism
Myelomeningocele and Myelocele.
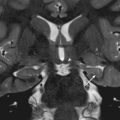
Incomplete or defective closure of the neural tube results in a neural placode that fails to detach from the adjacent surface ectoderm, a process termed nondisjunction. Consequently, a flattened midline neural placode is either flush with the cutaneous surface (myelocele-MC) or is pushed above or dorsal to the adjacent skin (myelomeningocele-MMC). MMC accounts for more than 98% of open spinal dysraphism. The prognosis of MMC and MC is worse than that of a skin-covered spinal dysraphism. MMC and MC have a significant impact on the quality of life. All children with an open spinal dysraphism have an associated Chiari II hindbrain malformation [ Fig. 9.1 ]. It is hypothesized that the chronic leakage of CSF at the level of the neural placode during the intrauterine development of the fetal brain results in an incomplete or defective expansion of the rhombencephalic vesicle. This in turn prevents normal growth of the skull base causing a small posterior fossa with herniation of hindbrain elements into the upper cervical spinal canal. Varying degrees of central canal dilation or frank hydromyelia may be present in the spinal cord in patients with MMC or MC. These malformations can be diagnosed by ultrasound during fetal life and confirmed by fetal MRI.

Hemimyelomeningocele and Hemimyelocele.
Hemimyelomeningoceles and hemimyeloceles are rare and are associated with diastematomyelia (cord splitting), and occur when one hemicord fails to undergo primary neurulation.
Closed (Skin-Covered) Spinal Dysraphism
Lipomyelomeningocele and Lipomyelocele.
Lipomyelomeningoceles (LMMC) and lipomyeloceles (LMC) have a significantly better neurologic prognosis than open neural tube defects, presumably because the neural placode is covered and protected by skin and subcutaneous tissue. LMMC and LMC are typically not associated with Chiari II malformation. Premature disjunction of the neural tube from the adjacent surface ectoderm before closure of the neural tube results in mesenchymal elements having access to the neural groove and ependymal lining of the grove. It is hypothesized that the interaction of mesenchymal elements with the inner lining of the neural tube induces an excess production of fat. On imaging, in lipomyeloceles, the neural tissue is flush with the spinal canal; in lipomyelomeningoceles, the neural tissue is pushed outside of the spinal canal with expansion of the subarachnoid space [ Fig. 9.2 ]. Large lipomas typically cover the neural placode and may extend from the subcutaneous region into the widened spinal canal.

Dorsal Dermal Sinus
Dorsal dermal sinuses are a distinct group of malformations that are classified as an intermediate between open and closed spinal dysraphisms. They are epithelial-lined fistulae or tracts connecting the skin surface with neural tissue or meninges. They are believed to result from a focal incomplete disjunction of the neuroectoderm from the surface ectoderm. Physical examination reveals a midline dimple or pinpoint ostium and may also reveal an associated hairy nevus, hyperpigmented patch, or capillary hemangioma. CSF may intermittently leak out of the ostium. The sinus tract may represent a port of entry for infections and may result in meningitis or abscess formation. The fistulous tract is well demonstrated on thin-slice, high-resolution T1- or T2-weighted sagittal images as a T1 hypointense, T2 hypointense, or hyperintense linear streak extending from the cutaneous dimple to the spinal canal [ Fig. 9.3 ]. The malformation may result in a low-lying spinal cord (ie, below the L2-3 disk level) and spinal cord tethering.

Disorders of Secondary Neurulation
Secondary neurulation is responsible for formation of the lowest part of the spinal cord including the conus medullaris and filum terminale. Secondary neurulation disorders include: (1) fibrolipoma of the filum terminale, (2) tight filum terminale syndrome, (3) caudal regression syndrome (CRS), and (4) sacrococcygeal teratoma (SCT).
Fibrolipoma of the Filum Terminale
Fibrolipomatous thickening of the filum terminale is referred to as a filar lipoma. However, filar thickening may be exclusively fibrous. Filar thickening, with or without fat, is a frequent normal finding on autopsy studies (4%–5%) and is only relevant if spinal cord tethering occurs. Tethered-cord syndrome is a clinical syndrome characterized by progressive neurologic abnormalities in the setting of traction on a low-lying spinal cord and conus medullaris. On imaging, a filar lipoma appears as a hyperintense strip or dot of signal on sagittal and axial T1-weighted images, respectively, within a thickened filum terminale [ Figs. 9.4 and 9.5 ]. Axial T2-weighted imaging is generally required to demonstrate fibrous thickening of the filum.


Tight Filum Terminale
Tight filum terminale syndrome is characterized by hypertrophy and shortening of the filum terminale. This condition causes tethering of the spinal cord and impaired relative ascent of the conus medullaris during development. The conus medullaris is low lying relative to its normal position, above the L2-L3 disk level [ Fig. 9.6 ].

Caudal Regression Syndrome
CRS is a spectrum of anomalies that have in common partial absence of lower vertebral elements and caudal spinal cord. CRS is associated with anorectal, lower-limb, and genitourinary malformations. In addition, CRS may be seen as part of the OEIS association (omphalocele, exstrophy, imperforate anus, spinal defects). The characteristic imaging findings are lack of the most distal segments of the spinal cord and matching musculoskeletal elements. Typically the spinal cord abruptly terminates with a club- or wedge-shaped inferior border [ Fig. 9.7 ]. The sacrum and coccyx are typically absent. The malformation can be categorized into two types depending on position and configuration of the conus medullaris: high and abrupt (type I) or low and tethered (type II).

Sacrococcygeal Teratoma
SCTs are the most frequently encountered large, congenital tumors in neonates and arise from the pluripotent cells of the caudal cell mass. SCTs occur more often in girls than in boys (3 : 1 ratio). SCTs are classified as types I to IV depending on the location of the mass. In type I the lesion is exclusively outside the pelvis, whereas in type IV it is entirely inside the pelvis. Prenatal ultrasound and fetal MRI allow identification and characterization (cystic vs. solid) of SCT [ Fig. 9.8 ]. Postnatal MRI is essential in the preoperative diagnostic workup to delineate the extension of tumor into the pelvis and degree of displacement or infiltration of pelvic structures.

Anomalies of Notochordal Development
Anomalies of notochordal development represent a complex dysraphism. These malformations may partially overlap with disorders of secondary neurulation (eg, CRS). These include the following entities: (1) split notochord syndrome, also known as diastematomyelia; (2) neurenteric fistula and (3) segmental disorders of notochordal development resulting in the previously described spectrum of CRSs; and (4) segmentation and formation anomalies of the vertebral column.
Diastematomyelia
The splitting of the spinal cord into two hemicords is referred to as diastematomyelia. The hemicords may be separated by either a membranous septum or a bony spur. Ectodermal cells that are encoded to glide between the ectoderm and endoderm do not remain in the midline but form two more laterally positioned hemi-notochords, which in turn induce the formation of two separate neuroectodermal layers resulting in two hemicords. Each hemicord has one ventral and one dorsal nerve root and one central canal. In addition, the two hemicords may either be located either within a single shared dural sac or in two distinct dural sacs [ Fig. 9.9 ]. Diastematomyelia is associated with formation and segmentation anomalies of the vertebral bodies. It is a skin-covered defect with associated cutaneous stigmata in 50% to 70% of patients. Up to 90% of patients have symptoms related to spinal cord tethering. The diagnosis should be made using fetal ultrasound or MRI. Postnatal MRI evaluates the spinal cord anatomy in detail. CT is especially helpful in the identification of a bony spur, if present.

Neurenteric Fistula
Neurenteric fistula is a rare malformation resulting from a persistence of the notochordal process. Consequently, there is a direct connection between derivates of the endoderm and the neuroectoderm resulting in a fistulous connection between the skin surface and bowel. Neurenteric cysts represent a more localized form of a neurenteric fistula and extend anteriorly.
Segmentation and Formation Anomalies of the Spinal Column
A spectrum of segmentation and formation anomalies may be recognized (1) as an incidental finding, eg on a plain radiograph of the chest or abdomen, with no neurologic compromise, (2) during the workup of scoliosis, and (3) as part of various syndromes and associations (eg, Klippel-Feil, VACTERL). Vertebral abnormalities result from a segmental derangement of the musculoskeletal somites. In addition to evaluating the bony anatomy, the contents of the spinal canal should be studied using MRI.
Other Developmental Abnormalities
Myelocystocele
Myelocystocele is an occult, skin-covered spinal dysraphism where the spinal cord with a dilated central canal and arachnoid protrude dorsally through a bony spine defect. Terminal myelocystoceles are believed to result from an abnormality of secondary neurulation, with an inability of CSF to exit from the early neural tube causing ballooning of the terminal ventricle of the conus placode into a cyst [ Fig. 9.10 ]. Nonterminal myelocystoceles result from partial failure of primary neurulation, with the presence of spinal cord parenchyma distal to the CSF-filled cyst, and frequently occur in the cervical or cervicothoracic regions.

Meningocele
Meningocele is an uncommon entity with herniation of a CSF-filled sac lined by dura and arachnoid matter beyond the spinal canal. No neural tissue is included in the meningocele [ Fig. 9.11 ]. The extension may be dorsal, lateral, or ventral.

Spondylodysplasias
Spondylodysplasia refers to any developmental abnormality of the bony spinal column. This category includes idiopathic scoliosis, congenital scoliosis and kyphosis, Scheuermann disease, and the skeletal dysplasias (eg, neurofibromatosis type 1 [NF-1], mucopolysaccharidoses [MPSs], spondyloepiphyseal dysplasia [SED], achondroplasia, and Down syndrome). An abnormality of the spinal curvature is a common presentation, based on clinical examination and CR, and includes scoliosis (lateral curvature), kyphosis (posterior angulation), and lordosis (increased anterior angulation). Skeletal dysplasias are a heterogeneous group of disorders in which there is abnormal cartilage and bone formation, growth, and remodeling. Compromise of the spinal canal/neural foramina and craniocervical instability, which may cause mechanical compression of the neural axis, are of major concern in skeletal dysplasias. CR, CT, and MRI play important roles in the evaluation of spondylodysplasias.
Idiopathic Scoliosis
Scoliosis is defined as a lateral curvature of the spine greater than 10 degrees on radiography and is typically associated with trunk rotation. The two major categories of scoliosis are idiopathic scoliosis and nonidiopathic scoliosis. Nonidiopathic scoliosis can be classified as (1) congenital scoliosis caused by malformation of vertebrae-like hemivertebra or block vertebra; (2) neuromuscular scoliosis caused by insufficiency of active muscular stabilizers of the spine, as in cerebral palsy, spinal muscular atrophy, spina bifida, muscular dystrophies, or spinal cord injuries; and (3) mesenchymal scoliosis caused by insufficiency of passive stabilizers of the spine, as in Marfan syndrome, mucopolysaccharidosis, or osteogenesis imperfecta. The diagnosis of an idiopathic scoliosis is made if a nonidiopathic cause has been excluded.
Idiopathic scoliosis (IS) is divided into three subcategories based on patient age: (1) infantile onset IS affects patients younger than 3 years, (2) juvenile onset IS occurs in children between 3 and 10 years of age, and (3) adolescent onset IS occurs in skeletally immature patients older than 10 years. Adolescent onset IS accounts for approximately 90% of cases of idiopathic scoliosis in children. The complications of IS include curve progression, cardiopulmonary compromise, painful curves, cosmetic deformity, neurologic dysfunction, and degenerative joint disease. Curve progression usually occurs during periods of growth acceleration. Treatment may be required and involves bracing or surgical instrumentation and fusion (eg, Harrington rods).
CR represents the gold standard in confirming the diagnosis and surveillance of IS. CT may be required for a preoperative evaluation [ Fig. 9.12 ]. The prevalence rate of CNS abnormalities in patients with IS is between 2% and 4%. The presence of an atypical curve pattern (left thoracic, absence of thoracic apical segment lordosis), abnormal neurologic finding (hyperreflexia, asymmetric deep tendon reflexes, urinary dysfunction, diminished rectal tone, or skin lesions over the lower back), and infantile or juvenile onset of scoliosis should prompt evaluation with MRI. MRI can show underlying abnormalities such as hydrosyringomyelia, tumor, cyst, or skin-covered spinal dysraphisms.

Congenital Scoliosis and Kyphosis
Congenital scoliosis occurs because of the presence of an underlying vertebral malformation. Vertebral malformations include hemivertebrae, vertebral bar (an abnormality of vertebral separation during development), butterfly vertebrae, and wedge-shaped vertebrae. Vertebral malformations may (1) present as an isolated finding; (2) occur in association with renal, cardiac, or spinal cord malformations; or (3) occur as part of an underlying syndrome or chromosomal abnormality [ Fig. 9.13 ]. Common syndromes associated with vertebral malformations are summarized in Table 9.1 . Other causes of kyphosis and kyphoscoliosis in childhood are postural, Scheuermann disease, neuromuscular disorder, trauma, inflammation, surgery, radiation therapy, metabolic disorders, arthritis, and tumor.