Solitary, well-defined, water density, unilocular cystic lesion
– Thin wall with sharp interface to normal splenic tissue
– No peripheral/intracystic enhancement or solid component
Some cysts can have septations, trabeculations, thick wall, internal necrotic debris, or calcification
– May have attenuation greater than simple fluid (due to hemorrhage or protein)
– Thin eggshell calcification or thick, irregular peripheral calcification
Congenital and acquired cysts may be indistinguishable
– Congenital cysts more likely simple in appearance
– Acquired cysts often complex with calcification
TOP DIFFERENTIAL DIAGNOSES
• Splenic infection and abscess
Pyogenic/fungal abscess or parasitic echinococcal cyst
• Splenic metastases and lymphoma
• Benign primary splenic tumors
• Intrasplenic pseudocyst
PATHOLOGY
• Congenital epidermoid (“true” cyst)
May be due to intrasplenic sequestration of peritoneal mesothelial cells during embryologic development
• Acquired cysts (secondary/“false” cysts or pseudocysts)
Due to prior trauma, hematoma, infarction, or infection
Majority of splenic cysts in North America due to prior trauma
Arise due to liquefactive necrosis and cystic change
CLINICAL ISSUES
• Most cysts discovered incidentally on imaging
• Small and asymptomatic: No treatment
• Symptomatic cysts usually treated, with options including percutaneous aspiration/drainage, cyst decapsulation or unroofing, and partial/complete splenectomy
Splenectomy for symptomatic large cysts (> 5 cm)
(Left) Axial CECT shows a water density mass with a calcified wall within the spleen. Note the absence of any enhancing or soft tissue components within this splenic cyst.
(Right) Postsplenectomy specimen in the same patient shows the calcified, fibrous wall of the cyst. This was an acquired cyst, probably as a result of prior trauma or infarction.
(Left) Coronal CECT in a young woman demonstrates a large, simple-appearing splenic cyst . The patient was symptomatic with pain and early satiety and consequently underwent surgical cyst deroofing.
(Right) Axial CECT demonstrates a large, nonenhancing, multiseptated splenic cyst replacing most of the spleen. Only a posterior sliver of normal spleen remains .
IMAGING
General Features
• Best diagnostic clue
Sharply defined, spherical cystic lesion of water density
• Key concepts
Classification
– Congenital epidermoid cysts (primary or “true” cyst)
Demonstrate inner cellular endothelial lining
Account for 10-25% of all splenic cysts
– Acquired cysts (secondary or “false” cysts)
No inner cellular lining, but have fibrous wall
Account for 80% of splenic cysts
Due to prior trauma, hematoma, or infarction
Development of cyst due to liquefactive necrosis
Radiographic Findings
• Curvilinear wall calcification in left upper quadrant
CT Findings
• Spectrum of appearances
Solitary, well-defined, water density unilocular cyst
– Thin wall with sharp interface to normal splenic tissue
– No peripheral or intracystic enhancement; no solid, nodular soft tissue component
– Always intraparenchymal (no exophytic component)
Some cysts can have septations, trabeculations, thick wall, and internal necrotic debris
– May have attenuation greater than simple fluid (due to hemorrhage or protein)
Cysts may have thin eggshell calcification or thick, irregular peripheral calcification
• Congenital and acquired cysts may be indistinguishable
Congenital cysts more likely to be simple in appearance
Acquired cysts more likely complex with calcification
MR Findings
• Most cysts are T2 hyperintense and T1 hypointense
• May have ↑ signal intensity on T1WI due to blood products or protein within cyst (especially if ↑ attenuation on CT)
Ultrasonographic Findings
• Anechoic with smooth margins and thin walls
Only gold members can continue reading. Log In or Register to continue
 Some cysts can have septations, trabeculations, thick wall, internal necrotic debris, or calcification
Some cysts can have septations, trabeculations, thick wall, internal necrotic debris, or calcification







 within the spleen. Note the absence of any enhancing or soft tissue components within this splenic cyst.
within the spleen. Note the absence of any enhancing or soft tissue components within this splenic cyst.

 . The patient was symptomatic with pain and early satiety and consequently underwent surgical cyst deroofing.
. The patient was symptomatic with pain and early satiety and consequently underwent surgical cyst deroofing.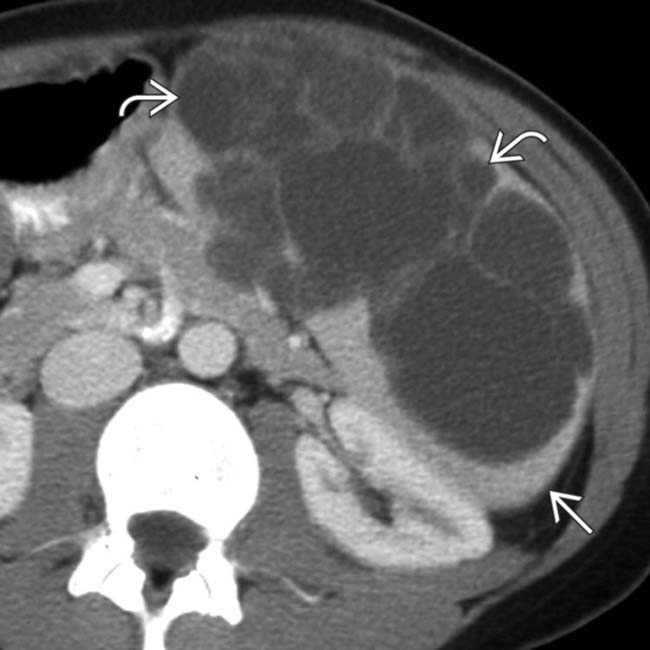
 replacing most of the spleen. Only a posterior sliver of normal spleen remains
replacing most of the spleen. Only a posterior sliver of normal spleen remains  .
.
















