Fig. 1
A typical 5 × 5 cm field used for conventional radiotherapy with opposed laterals for T1N0 glottic carcinoma

Fig. 2
A patient with T1N0 squamous cell carcinoma of the left vocal cord. Because of the low rate (<5 %) of nodal metastases for early-stage glottis cancer, there is no elective nodal irradiation. Please note that these are representative slices and not all slices are included. Blue = GTV, Green = CTV, Red = PTV. GTV is delineated by laryngoscopy findings only. For T1 larynx tumors, there are typically no CT abnormalities. The entire larynx is delineated as CTV to include both false and true vocal cords, anterior and posterior commissures, arytenoids and aryepiglottic folds, as well as the subglottic region. The PTV extends from thyroid notch to the bottom of the cricoid cartilage. A 5 mm margin is added in all directions except posterolaterally where it is limited to 3 mm to spare the carotid artery

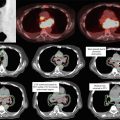
Fig. 3
A patient with T2N0 squamous cell carcinoma of the right vocal cord with subglottic extension. Yellow = GTV, Orange = CTV, Red = PTV. GTV is delineated by laryngoscopy findings only. The entire larynx is delineated as CTV to include both false and true vocal cords, anterior and posterior commissures, arytenoids and aryepiglottic folds, as well as the subglottic region. Note in these images, the piriform sinuses are included in the CTV, as has been the historical practice at our institution. However, given that the piriform sinuses are not part of the true larynx, they may be excluded from the CTV to enhance carotid sparing. The PTV extends from thyroid notch to the bottom of the first tracheal ring inferiorly. A 1 cm margin is added in all directions except posterolaterally, where it is reduced to as little as 3 mm to exclude the carotid artery
An alternative to conventional radiotherapy is carotid-sparing IMRT (Gomez et al. 2010; Rosenthal et al. 2010; Chera et al. 2010). For IMRT, a GTV should be delineated to encompass all suspicious lesions identified from laryngoscopy and imaging studies. The CTV should encompass the entire larynx, including the both the anterior and posterior commissures and the arytenoids. Although the inferior piriform sinuses are not part of the target volume, they are often included in the CTV at our institution given the relatively small increase in total volume. The PTV is typically a 0.5–1 cm three-dimensional expansion on the CTV, although the margin may be reduced to as little as 0.3 cm near the carotid arteries. The superior and inferior borders should be similar to the respective borders used in conventional radiotherapy. The superior extent of the PTV should extend to the thyroid notch. The inferior extent of the PTV varies depending on the tumor stage. For T1N0 tumors, generally the inferior border of the PTV is the bottom of the cricoid. For T2N0 tumors, especially if there is subglottic extension, the inferior border of the PTV should be extended an additional 1 cm to include the first tracheal ring. In general, the PTV should also extend a minimum of 2 cm above and below the GTV (Table 1).
Table 1




Suggest target volumes for carotid-sparing IMRT in early-stage glottic carcinoma
Related posts:





Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
