2 The central nervous system
Cerebral cortex (Figs 2.1, 2.2)
The superolateral surface of each cerebral hemisphere has two deep sulci; these are:
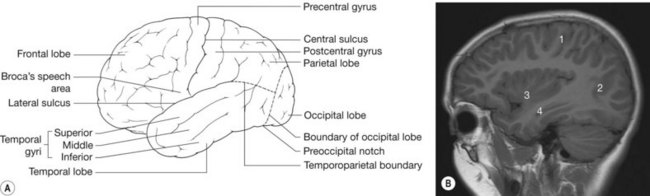
Figure 2.1 • (A) Superolateral surface of the cerebral hemisphere. (B) Sagittal MRI of brain lateral to midline.
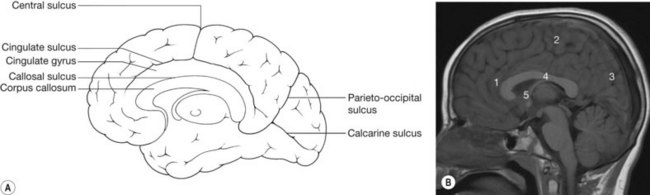
The parieto-occipital sulcus on the medial surface of the hemisphere separates the parietal and occipital lobes. On the lateral surface of the hemispheres there is no complete sulcal separation of the parietal, temporal and occipital lobes. The boundary between the parietal and temporal lobes lies on a line extended back from the lateral sulcus. The boundary separating the parietal and temporal lobes from the occipital lobe is a line between the superior border of the parieto-occipital sulcus and the preoccipital notch (see Fig. 2.1).
Parietal lobe
The parietal lobe is posterior to the central sulcus, superior to the lateral sulcus and a line drawn from its posterior end to the occipital lobe (see Fig. 2.1). Areas with known function include the sensory cortex and the parietal association cortex.
Occipital lobe
The occipital lobe lies posterior to the parietal and temporal lobes. There is no anatomical separation of these lobes on the superolateral surface of the hemisphere. However, on the medial surface the occipital lobe is separated from the parietal lobe by the parieto-occipital sulcus. A further deep sulcus of this surface, the calcarine sulcus, runs anteriorly from the occipital pole (see Fig. 2.2). Areas with known function include the visual cortex and the occipital association cortex.
Radiological features of the cerebral cortex
CT and MRI
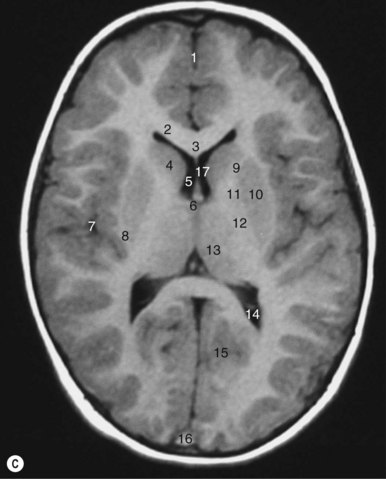
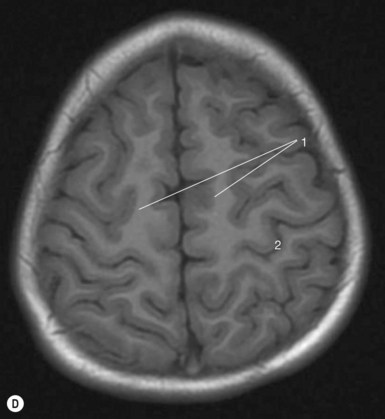
Identification of lobes on CT slices depends on identification of their boundaries. The sylvian cistern and fissure separating the frontal and temporal lobes are easily identified on axial CT or MR slices (Fig. 2.3). The central sulcus that forms a boundary between the frontal and parietal lobes is less well seen, however. This lies at a transverse level just posterior to the anterior limit of the lateral ventricles. Because CT images are obtained parallel to the canthomeatal line, on upper images the central sulcus is quite posterior in position. On axial images it has been described as having an inverted omega shaped curve that marks the position of the hand motor cortex (Fig. 2.3D).
The parieto-occipital sulcus on the medial surface of the hemisphere can be seen on CT at the level of the lateral ventricles and on midline sagittal MR images (see Fig. 2.5). The parieto-occipital junction on the lateral surface has no anatomical landmark but lies at approximately the same transverse level as the sulcus.
White matter of the hemispheres
There are three types of fibre within the cerebral hemispheres:
Commissural fibres
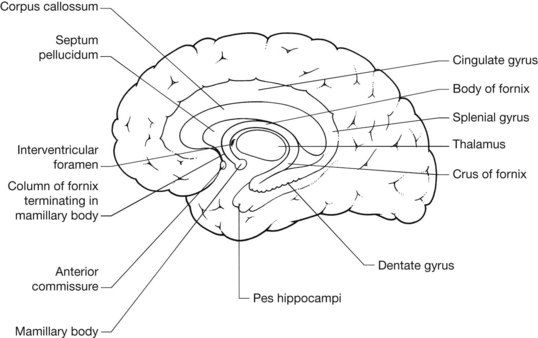
The corpus callosum (Figs 2.4, 2.5)
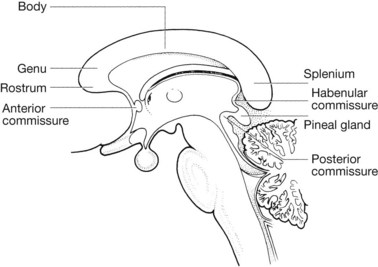
Posterior commissure
This is situated anterior and inferior to the pineal body. It connects the superior colliculi, which are concerned with light reflexes (see brainstem).
Radiological features of the commissural and projection fibres
CT and MRI
The corpus callosum cannot be well seen on axial CT slices. The internal capsule is seen as a V-shaped low-attenuation or high T1 signal structure (see Fig. 2.3C) between the caudate and lentiform nuclei anteriorly and the lentiform and thalamus posteriorly.
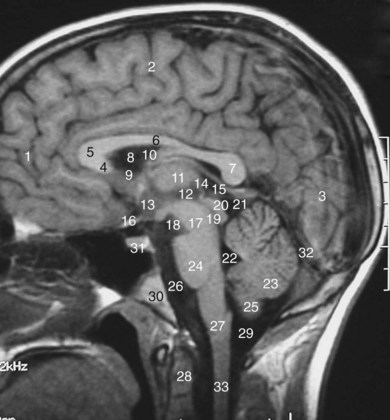
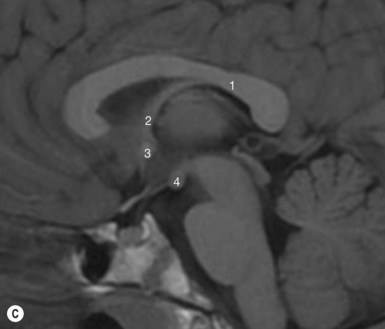
The rostrum, genu, body and splenium can be seen on sagittal MRI (Fig. 2.5). The anterior and posterior commissures can also be seen on this view. A line joining the anterior and posterior commissures, the AC–PC line, is used as a reference in image-guided procedures.
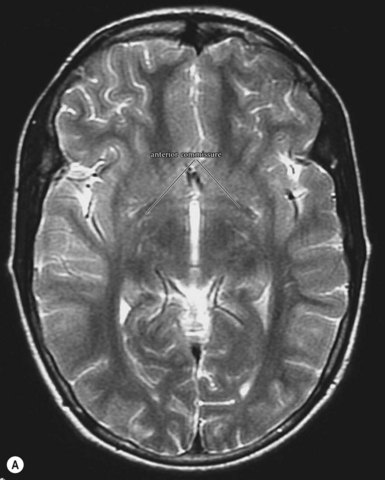
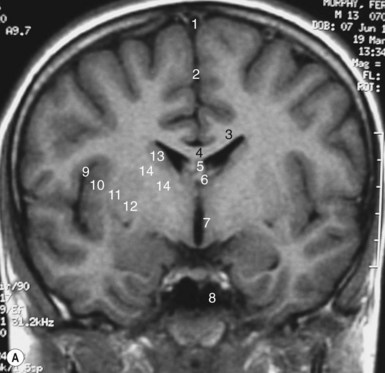
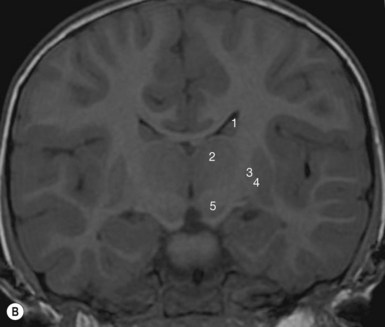
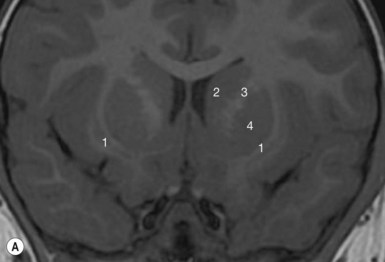
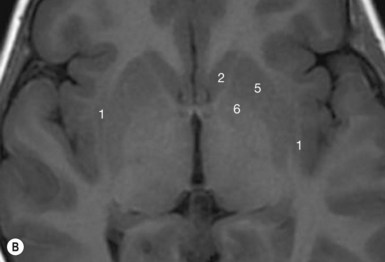
On coronal MRI scans (Fig. 2.7) the body of the corpus callosum and the tapetum can be seen superior to the lateral ventricles and the internal capsule can be seen lateral to the thalami. On this view the anterior commissure may also be visible inferior to the third ventricle, but this commissure is best seen as an arc of fibres on axial MRI (Fig. 2.6).
Radiology pearl
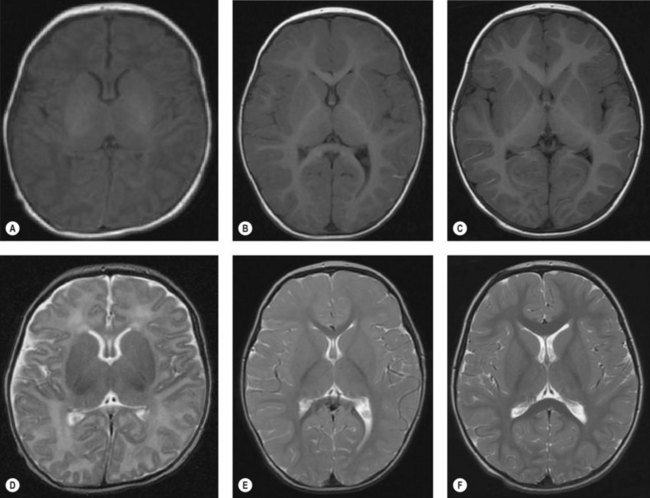
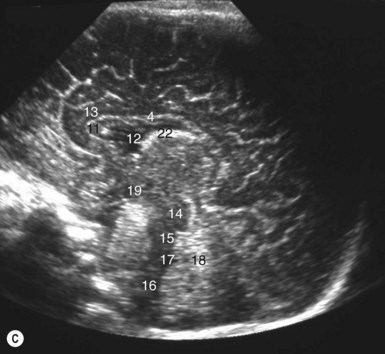
Unmyelinated immature white matter because of its higher water content is darker on T1 sequences and brighter on T2 sequences than mature myelinated white matter. The progression of myelination can therefore be seen on MRI of infants. This progresses in a predictable way from deep to superficial, from posterior to anterior and from inferior to superior (Fig. 2.8)
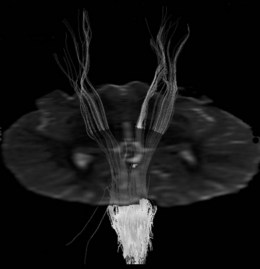
MR tractography is a technique that uses diffusion tensor imaging to obtain images of fibre tracts within the brain. These scans also give information about fibre direction (Fig. 2.9).


Basal ganglia (Figs 2.11, 2.12)
This subcortical grey matter includes:

Radiological features of the basal ganglia
CT and MRI
On axial CT or MRI the head of the caudate nucleus can be seen projecting into the anterior horn of the lateral ventricle on slices taken at ventricular level (see Fig. 2.3C). The head of the caudate nucleus is usually more radiodense than the lentiform nucleus or the thalamus, especially in older subjects. The body of the caudate nucleus is seen as a thin, dense stripe on the superolateral margin of the lateral ventricle on higher cuts, where it should not be confused with heterotopic cortical tissue.
The claustrum can be seen on MRI (Fig. 2.12) as a high-attenuation stripe, separated from the putamen by the external capsule and from the insula by the extreme capsule.
The amygdala is an ovoid mass of grey matter at the anterior end of the tail of the caudate nucleus and can be seen on MRI anterior to the hippocampus in the medial temporal lobe (Fig. 2.11 and 2.16C).
Thalamus, hypothalamus and pineal gland
Thalamus
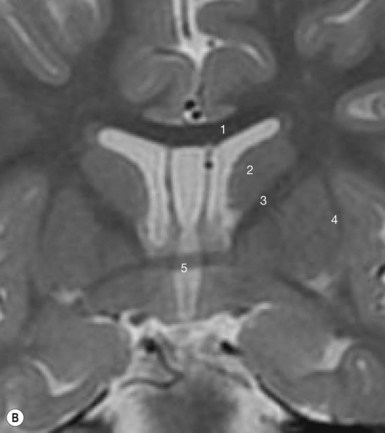
Separate to and below the thalami are paired nuclei called the subthalamic nuclei (Fig. 2.7B) which are connected to the lateral putamen and the substantia nigra. Their function is unknown but destruction of one of them causes hemiballismus.
Hypothalamus (Figs 2.13, 2.21)
Radiological features of the thalamus, hypothalamus and pineal gland
CT and MRI
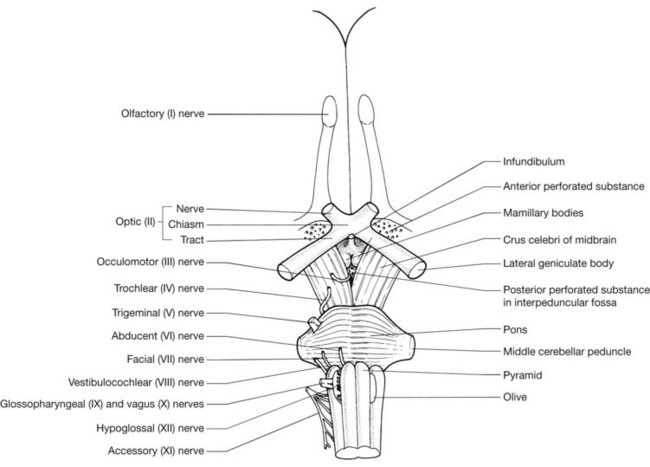
The structures forming the hypothalamus can best be appreciated on midline sagittal MRI (Fig. 2.5). The optic chiasm, the tuber cinereum, the infundibular stalk and the interpeduncular cistern, containing the mamillary bodies and in the base of which lies the posterior perforated substance, can be identified. The thalami can be seen on axial images on each side of the third ventricle (Fig. 2.3C). Their relationship to the posterior limb of the internal capsule and to the lentiform nucleus can be appreciated on this slice. The pineal gland and its superior and inferior laminae can also be best seen on midline sagittal MRI. Subthalamic nuclei can best be seen on coronal MRI (Fig. 2.7B).
Pituitary gland (Fig. 2.14)
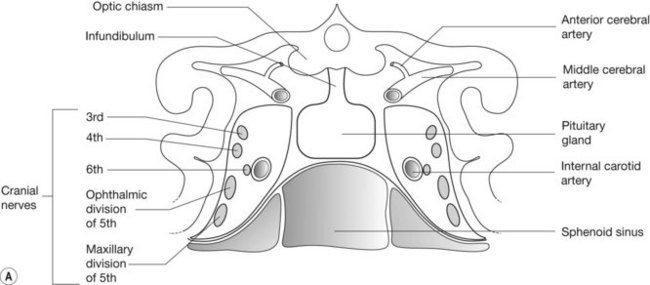
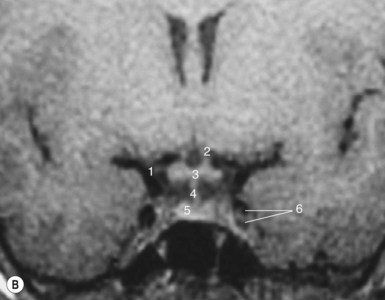
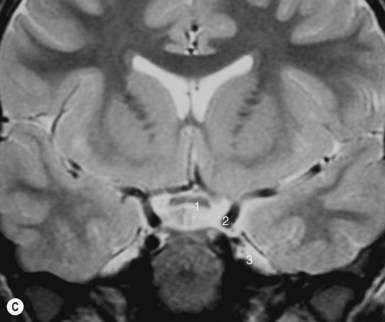
The relations of the pituitary gland are as follows: