3 The spinal column and its contents
The vertebral column
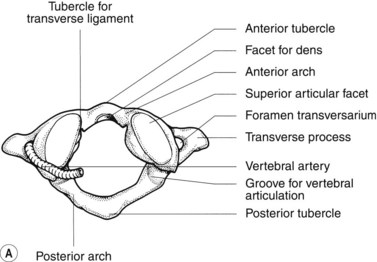
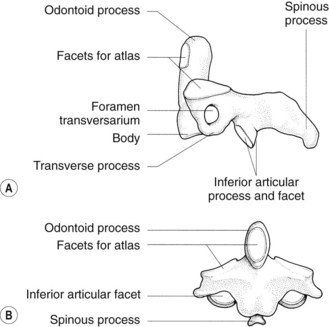
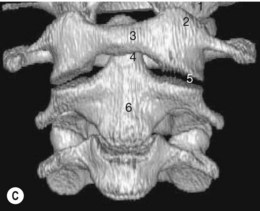
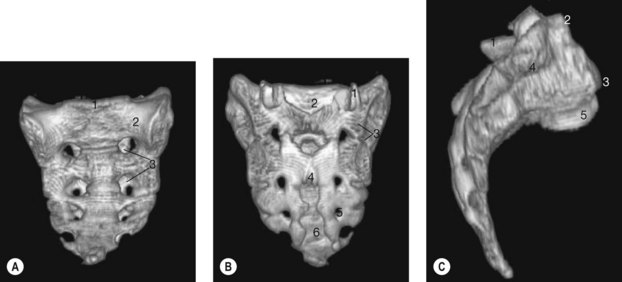
A typical vertebra (Figs 3.1, 3.4, 3.5)
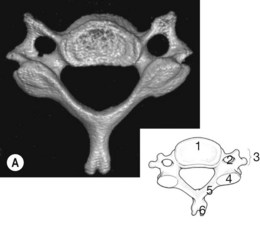
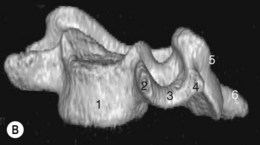
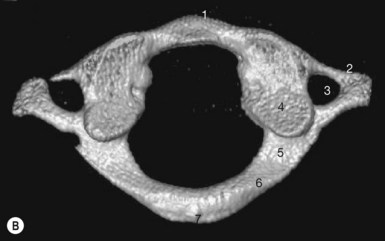
Figure 3.1 • Cervical vertebra. (A) 3D CT cervical vertebra viewed from above. (B) 3D CT cervical vertebra anterolateral view.
The cervical vertebrae
The thoracic vertebrae (Fig. 3.4)
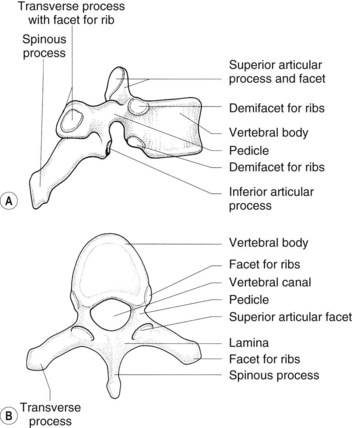

The spinous processes of the thoracic vertebrae are long and slope downwards.
The facets on the articular processes are relatively vertical.
The lumbar vertebrae (Fig. 3.5)
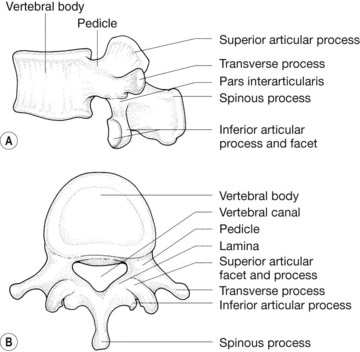
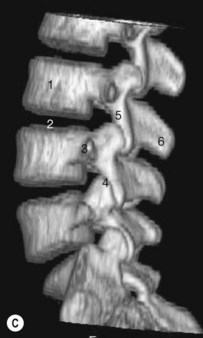
Figure 3.5 • Typical lumbar vertebra. (A) Lateral view. (B) Superior view. (C) 3D CT of lumbosacral spine.
The transverse processes of the upper four lumbar vertebrae are spatulate and increase in size from above downwards. The transverse process of the fifth lumbar vertebra is shorter but strong and pyramidal and, in contrast to those of the other vertebrae, does not arise from the junction of the pedicle and lamina but from the lateral aspect of the pedicle and the vertebral body itself (Fig. 3.5C).
The sacrum (Fig. 3.6)
Differences in the sacrum between male and female include:
Radiological features of the vertebrae
Radiographs of the vertebral column (Figs 3.7–3.9)


Radiographs of the cervical spine
In basilar invagination these relationships are abnormal.
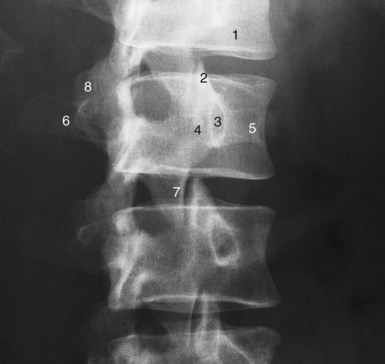
Radiographs of the lumbar spine
Oblique views of the lumbar spine (see Fig. 3.9) are used to visualize the intervertebral foramina and the pars interarticularis.
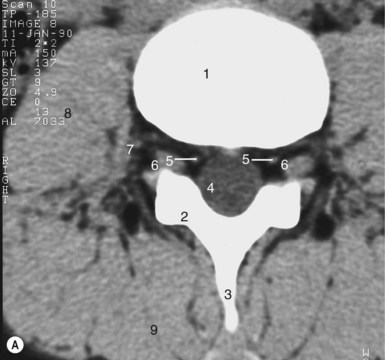
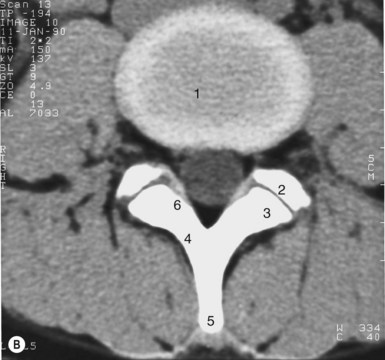
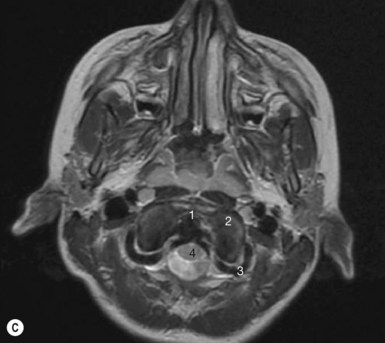
Computed tomography (Figs 3.1–3.6 and 3.10)