6 The pelvis
The bony pelvis, muscles and ligaments (Figs 6.1–6.7)
The pelvis (Fig. 6.1A, B) is a bony ring consisting of paired innominate bones, the sacrum and coccyx. The innominate bones articulate with each other anteriorly and with the sacrum posteriorly. Each innominate bone is composed of three parts, which fuse at the acetabulum.
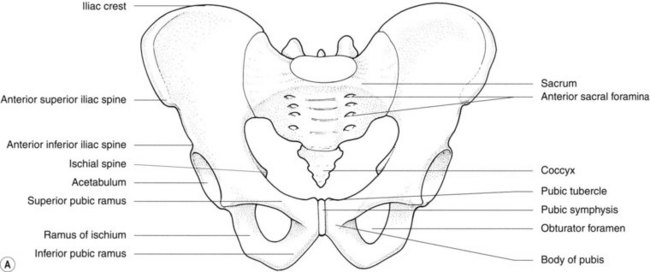
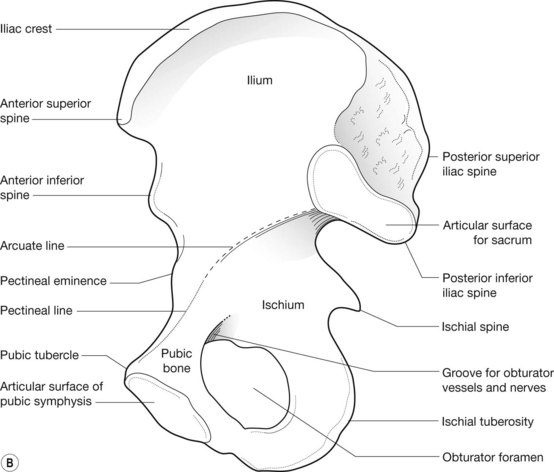
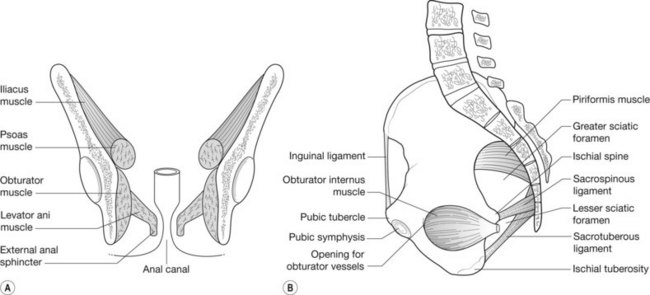



Figure 6.5 • MRI pelvis – coronal section through male pelvis: (A) anterior section; (B) posterior section.
The sacroiliac joints
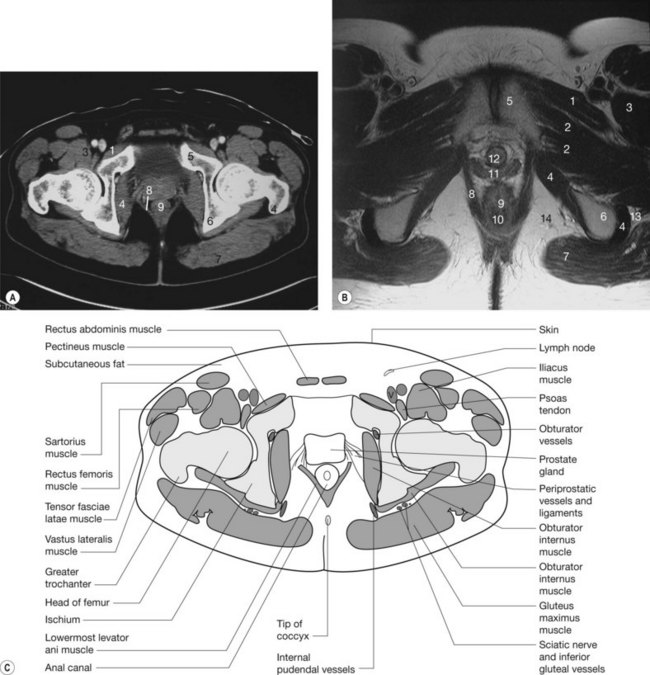
The pelvic muscles are shown in Figure 6.2. At the level of the iliac crest the paired psoas muscles lie on either side of the spine. They descend anteriorly, fusing with the iliacus muscle, which arises from the inner surface of the ilium. The fused iliopsoas muscle passes anteriorly under the inguinal ligament to insert into the lesser trochanter of the femur.
Radiology of the pelvic ring
Plain films
The bony landmarks may be identified on the plain radiograph (Fig. 6.3). The sacral promontory and superior part of the pubic bone define the pelvic inlet and the iliopectineal line running between separates the true pelvis below from the false pelvis above. The sacroiliac joints are not optimally seen on the frontal view owing to their obliquity. Special views may be performed so that the X-ray beam passes through the joint to demonstrate it clearly.
The pelvic floor (Figs 6.5–6.7; see also Figs 6.17, 6.21–6.25, 6.27, 6.28)
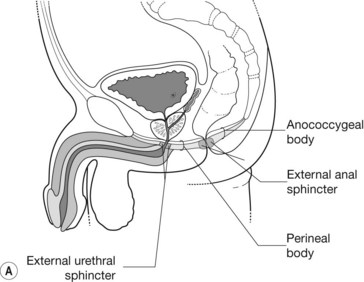
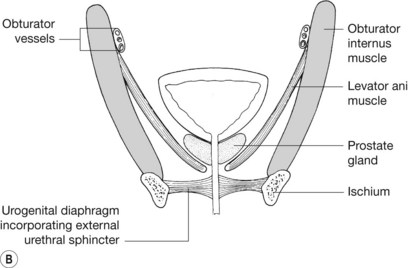
Figure 6.7 • Male pelvis: (A) sagittal section showing pelvic floor and urethra; (B) coronal section showing the pelvic floor.
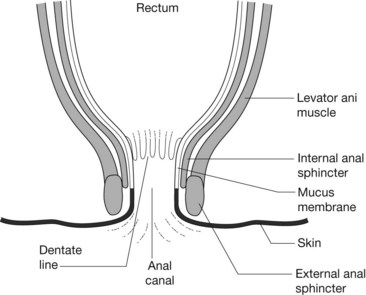
The levator ani muscle is the principal support of the pelvic floor. It provides muscular support for the pelvic organs and reinforces the urethral and rectal sphincters. Levator ani arises in a line from the posterior aspect of the superior ramus of pubis to the ischial spine. Between these bony points, the muscle arises from the fascia covering the obturator internus muscle on the inner wall of the ilium in an arc known as the tendinous arch or white line (Fig. 6.5A). Its fibres sweep posteriorly, inserting into the perineal body (a fibromuscular node behind the urethra in males or the urethra and vagina in females), the anococcygeal body (a fibromuscular node between the anus and coccyx) and the lowest two segments of the coccyx. The midline raphe of the levator ani anterior to the coccyx is also known as the levator plate. The fibres of levator ani sling around the prostate gland or vagina and rectum, blending with the external anal sphincter (Fig. 6.5B).
The posterior compartment is the anal triangle. It contains the anus and its sphincters, with the ischiorectal fossa on either side. The ischiorectal fossa is the space below and lateral to the posterior part of levator ani and medial to the inner wall of the pelvis (Fig. 6.5). It is bounded posteriorly by sacrotuberous ligaments and the gluteus maximus muscle, laterally by the fascia of the obturator internus muscle and anteriorly by the perineal body. It contains mainly fat.
The sigmoid colon, rectum and anal canal (Figs 6.8, 6.9; see Fig. 5.19)
The sigmoid colon
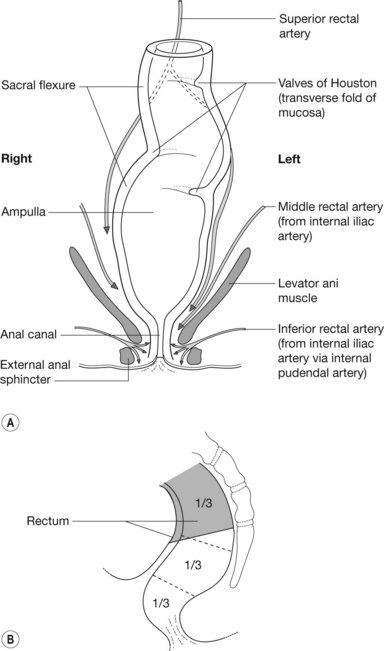
Figure 6.8 • Rectum: (A) anterior view and blood supply; (B) lateral view showing peritoneal reflections.
Radiology of the sigmoid and rectum
Magnetic resonance imaging
MRI is also used to image the rectum. Coronal and sagittal images are used to assess tumour spread and to evaluate the mesorectal fat (see Figs 6.5, 6.17) in rectal tumours.
Blood vessels, lymphatics and nerves of the pelvis
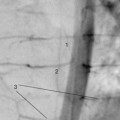
Internal iliac artery (Figs 6.10, 6.11)
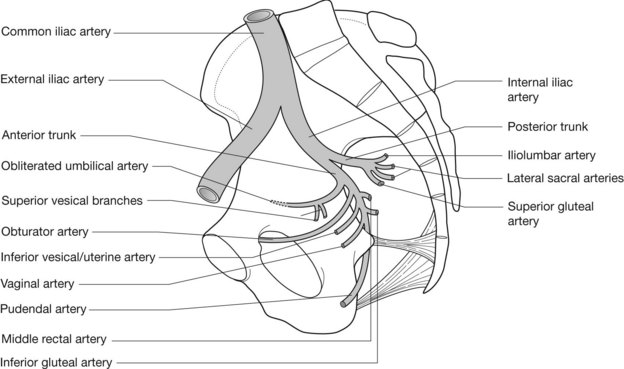
Branches of the anterior trunk
Branches of the posterior trunk
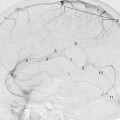
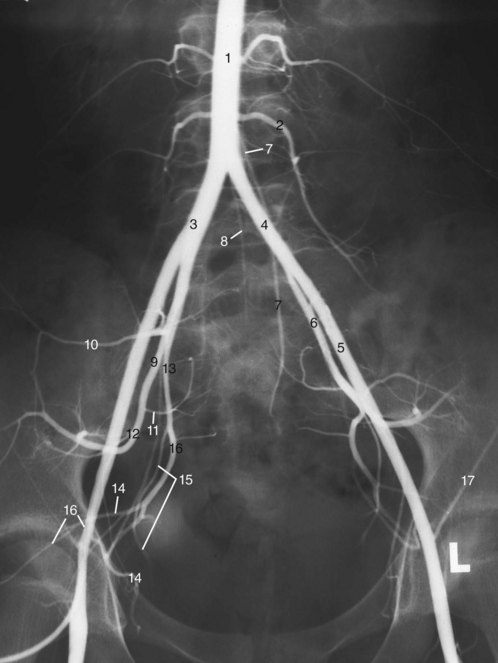
Radiology pearls (Fig. 6.13)