8 The lower limb
The bones of the lower limb
The femur (Fig. 8.1; see also Fig. 6.1)
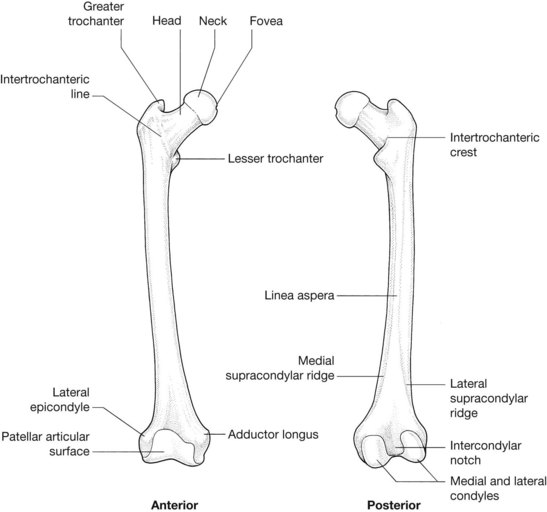
Radiological features of the femur (see Fig. 6.1)
Plain radiographs
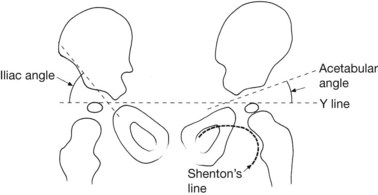
A line along the inferior margin of the neck of the femur forms a continuous arc with the superior and medial margin of the obturatur foramen of the pelvis. This line, known as Shenton’s line (see Fig. 8.8), is disrupted in congenital dislocation of the hip.
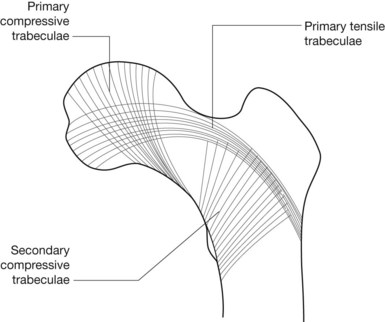
Trabecular markings in the neck of femur and bone density
Additional biomechanical integrity of the neck of the femur is provided by an ordered internal trabecular network with a combination of primary compressive trabeculae, primary tensile trabeculae and secondary compressive trabeculae. These trabeculae, readily identified on conventional radiographs, surround a triangular area where there is a relative paucity of trabecular markings, termed Ward’s triangle. The integrity of these described trabeculae reflects relative osteoblastic activity and stress. In osteoporosis, the disappearance of secondary compressive trabeculae prior to the disappearance of primary tensile trabeculae prior to subsequent disappearance of primary compressive trabeculae forms the basis of the Singh index (Fig. 8.2).
Radiological features of the patella
Dislocation of the patella
Wiberg describes three shapes of patella:
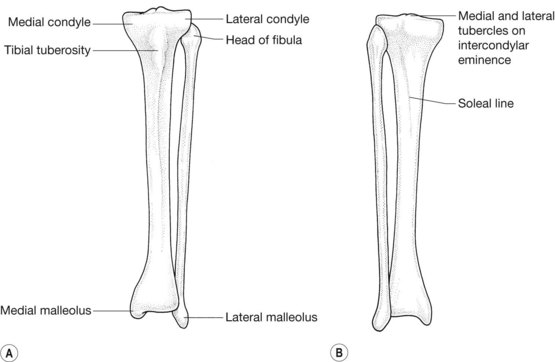
Radiological features of the tibia and fibula
The bones of the foot (Figs 8.4, 8.5)
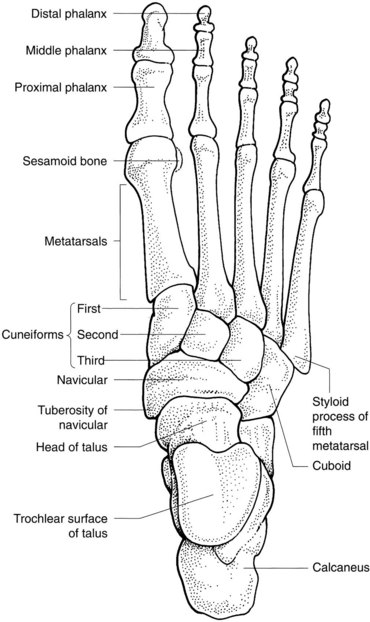

The talus
The inferior surface of the talus (see also the subtalar joint) has a large facet posteriorly for articulation with the calcaneus. Separated from this by the sinus tarsi are three facets, separated by ridges, as follows:
Radiological features of the bones of the foot (Fig. 8.6)
Plain radiographs
Boehler’s critical angle of the calcaneus (see Fig. 8.6A) is the angle between a line drawn from the posterior end to the anterior end of its superior articular facet and a second line from the latter point to the posterosuperior border of the calcaneus. It is normally 30–35°, with an angle less than 28° occurring when there is significant structural damage to the bone.
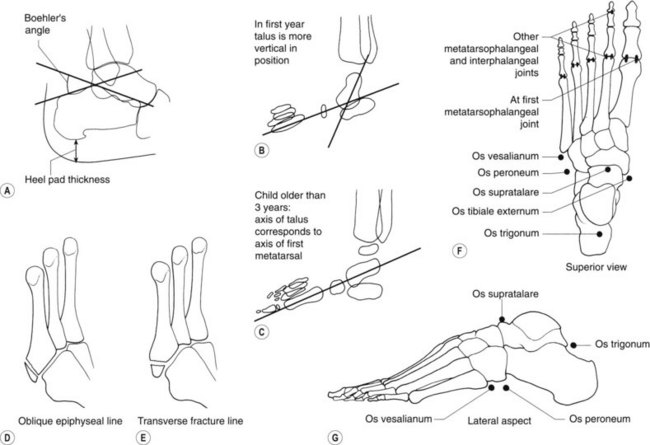
Heel-pad thickness (see Fig. 8.6A) is measured on a lateral radiograph of the calcaneus between the calcaneal tuberosity posteroinferiorly and the skin surface. Normal thicknesses are 21 mm in the female and 23 mm in the male. Thickening of the heal pad occurs in patients with gigantism or acromegaly.
On a lateral radiograph of the foot in children over 5 years old the long axis of the talus points along the shaft of the first metatarsal. In the younger child the talus is more vertical and its long axis points below the first metatarsal (see Fig. 8.6B, C).
Radiology pearl
The peroneus brevis tendon is attached to the styloid process of the base of the fifth metatarsal. The oblique epiphyseal line here should not be confused with a fracture of the styloid process, which is usually transverse, termed a Jones fracture (see Fig. 8.6D, E).
Sesamoid bones
The commonest sesamoid bones seen in foot radiographs (see Fig. 8.6F, G) are as follows:
The joints of the lower limb
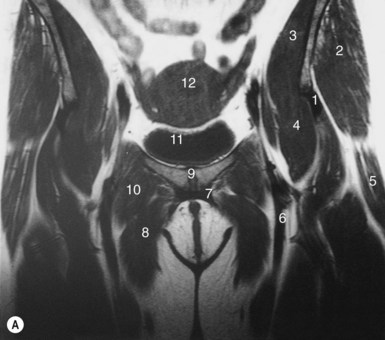
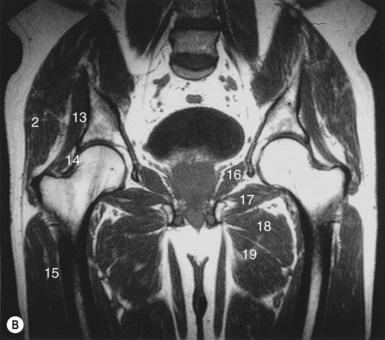
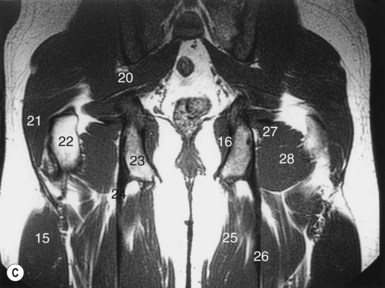
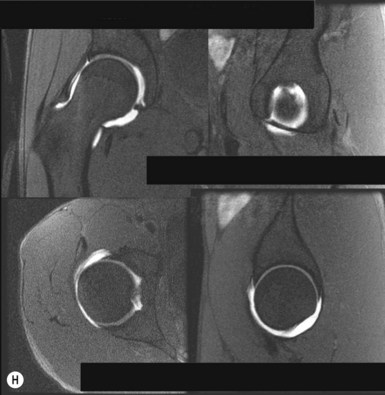
The hip joint (Fig. 8.7)
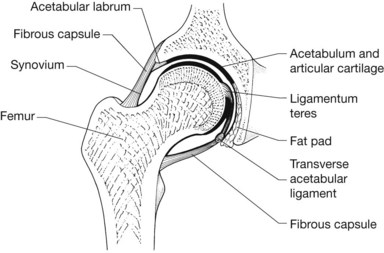
Radiological features of the hip joint
Plain radiographs
Similarly, irregularity of the superior margin of the acetabulum in children is a normal variant.
In assessment of radiographs of the hip in infants (Fig. 8.8), the following lines and angles are as described:
In assessment of radiographs of the adult hip, routine frontal radiographs allow the identification of six lines (see Fig. 6.3). The continuation of the inferior margin of the superior pubic ramus superiorly to the upper outer margin of the acetabular roof forms the outer margin of the anterior column or wall of the acetabulum (line 1). The continuation of the inferior margin of the inferior pubic ramus superiorly to the upper outer margin of the acetabular roof forms the outer margin of the posterior column or wall of the acetabulum (line 2). The continuation of the superior margin of the superior pubic ramus superiorly forms the iliopectineal line (line 3). The continuation of the superior margin of the inferior pubic ramus superiorly forms the ilioischial line (line 4). The roof of the acetabulum forms line 5. The ‘tear drop’ is formed by the reflections of the cotyloid fossa and quadrilateral plate and represents line 6. Disruption of any of the described lines is employed in the localization of disease processes on conventional radiographs.
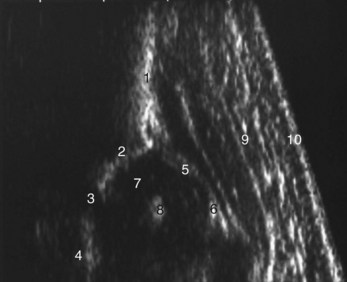
Ultrasound of the infant hip (Fig. 8.9)