The Infant Hip Joints
Charlotte Henningsen
|

OBJECTIVES
Describe the embryologic development of the hip joint.
Illustrate the bones and joints of the hip.
List the risk factors associated with the developmental dysplasia of the hip.
Define the process for sonographic evaluation of the hip.
Describe the etiologies of hip effusion.
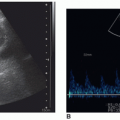
Identify the sonographic appearance of hip effusion.
Define proximal femoral focal deficiency.
KEY TERMS
developmental dysplasia of the hip
hip effusion
proximal femoral focal deficiency
septic arthritis
transient synovitis
GLOSSARY
abduct
to move away from the midline
to move away from the midline
adduct
to move toward the midline
to move toward the midline
arthrocentesis
to remove fluid from a joint through a needle
to remove fluid from a joint through a needle
arthroplasty
joint replacement
joint replacement
erythrocyte sedimentation rate
a nonspecific indicator for inflammation; a measurement of the time it takes for red blood cells to settle in a tube of unclotted blood
a nonspecific indicator for inflammation; a measurement of the time it takes for red blood cells to settle in a tube of unclotted blood
mesoderm
the middle germ cell layer that contributes to the embryologic development of connective tissue, bone, blood, muscle, vessels, and lymphatics
the middle germ cell layer that contributes to the embryologic development of connective tissue, bone, blood, muscle, vessels, and lymphatics
osteomyelitis
infection of the bone marrow and bone
infection of the bone marrow and bone
torticollis
a head that is held sideways owing to a muscle contraction
a head that is held sideways owing to a muscle contraction
Developmental dysplasia of the hip (DDH) describes a range of dysplasia that includes instability, subluxation, and frank dislocation. DDH was previously known as congenital dysplasia of the hip, but most dislocations occur after birth. The overall frequency of DDH is 20:1,000 live births, with dislocations occurring in 1 to 2 out of 1,000 births, and many of the milder manifestations resolve spontaneously shortly after birth.1 Early diagnosis and treatment are important to avoid significant and permanent disability. Clinical assessment and sonography are the two most common methods utilized in the detection of DDH.2 This chapter provides an overview of the development and anatomy of the hip and explores the risk factors associated with DDH. Sonographic evaluation for DDH is explained in addition to other diseases that can affect the hip, including hip effusion and focal femoral deficiency.
EMBRYOLOGY
There are three germ layers from which all body systems form: the ectoderm, the mesoderm, and the endoderm. The bones, connective tissues, and muscles are derived from the mesoderm. The initial development of the mesoderm occurs in the latter part of the third week postconception, which marks the beginning of bone formation. From the mesoderm, mesenchymal cells arise that are concentrated in
the cephalic end of the body and, along with cells derived from the neural crest, contribute to the development of the face and head. The ossification of the bones of the arms and legs begins at the end of the third week, which marks the end of the embryonic period, although the development of bones continues into adult life. Initially, the limbs arise as buds with the distal ends developing into paddle-like structures from which the bones continue to develop and fingers and toes arise. Myoblasts differentiate to develop into the muscles of the long bones. The joints of the body begin to develop during the sixth week, and during the seventh week of development, the upper and lower limbs will rotate on their longitudinal axes.3
the cephalic end of the body and, along with cells derived from the neural crest, contribute to the development of the face and head. The ossification of the bones of the arms and legs begins at the end of the third week, which marks the end of the embryonic period, although the development of bones continues into adult life. Initially, the limbs arise as buds with the distal ends developing into paddle-like structures from which the bones continue to develop and fingers and toes arise. Myoblasts differentiate to develop into the muscles of the long bones. The joints of the body begin to develop during the sixth week, and during the seventh week of development, the upper and lower limbs will rotate on their longitudinal axes.3
ANATOMY
The bones of the hip joint are composed of the pelvic girdle and the femur. The hip bone or coxal bone is composed of the ilium, ischium, and pubis (Fig. 23-1). The acetabulum is located at the lateral aspect of these bones and is joined by a growth plate, the triradiate cartilage. This creates an articulation point for the femur. The proximal aspect of the femur, the femoral head, is rounded and sits in the acetabulum. At the rim of the acetabulum sits a lip of cartilage called the acetabular labrum (Fig. 23-2). The femoral head is contiguous with the neck, which is contiguous with the diaphysis or shaft of the femur. The femoral head is cartilaginous at birth and the acetabulum is composed of cartilage and bone. The femoral head begins to ossify from the center outward at 2 to 8 months of age (Fig. 23-3).4 The cartilaginous characteristics allow for sonographic evaluation of the hip in infants. It is also because of the large cartilaginous component of the hip that it is subject to molding with normal development dependent on the femur being in good contact with the acetabulum. Additionally, during fetal development, maternal hormonal influences contribute to the laxity of fetal ligaments, which may in turn create a vulnerable atmosphere for the hip to become subluxable or dislocatable.
 FIGURE 23-1 Hip joint anatomy. The illustration of the anterior hip joint shows the ilium, ischium, and pubis forming the hip bone. The acetabulum is located at the lateral aspects and has the triradiate cartilage (growth plate), which creates an articulation point for the femoral head. |
DEVELOPMENTAL DYSPLASIA OF THE HIP
DDH occurs most frequently at birth but may also appear throughout infancy. The cause may be mechanical as a result of positional influences in utero and after birth, or the cause may be physiologic—resulting from a response to maternal hormones in utero or physical makeup after birth.
Risk Factors
Several risk factors have been identified for DDH, including breech birth and positive family history, especially if a parent or sibling is affected.5 High birth weight, multiple gestations, knee dislocations, limited abduction, and increased gestational weeks at birth are also risk factors. Torticollis and clubfoot have also been identified. Tight swaddling of infants with legs extended and adducted has also be implicated as a causative factor.6 The left hip has been identified as being more commonly affected than the right.7 Conversely, there are protective factors that guard against DDH including decreased birth weight and premature delivery.6 Education in appropriate swaddling techniques has also greatly reduced the risk of DDH in those populations.
Clinical Assessment
A routine neonatal screening typically includes clinical assessment of both hips. The assessment should be completed by experienced hands and when the infant is relaxed. Even in experienced hands, sonographic evaluation may detect instabilities that are undetected by clinical examination; however, research has shown that many of these dysplasias will become normal without treatment.2 More significant dysplasias can lead to osteoarthritis, low back pain, disability, and diminished quality of life and require surgical treatment, including hip arthroplasty in adult life.1 A proper diagnosis, which results in the best treatment plan, is dependent on the expertise of the individual examining the infant.
Barlow and Ortolani Maneuvers
The Barlow and Ortolani tests are two maneuvers for assessing hip stability. With the Barlow maneuver, the examiner attempts to push the femoral head posteriorly out of the socket, and with the Ortolani maneuver, the examiner attempts to reduce a recently dislocated hip.
The Barlow provocative maneuver test is performed on a supine infant with legs flexed at 90 degrees. The examiner grasps the symphysis pubis and sacrum with one hand while the other hand is placed over the knee area and adducts the leg. Slight outward pressure is then exerted over the
knee and distal thigh area in an effort to dislocate the hip. A palpable sensation of movement called a clunk is felt as the femoral head exits the acetabulum posteriorly.5,8,9
knee and distal thigh area in an effort to dislocate the hip. A palpable sensation of movement called a clunk is felt as the femoral head exits the acetabulum posteriorly.5,8,9
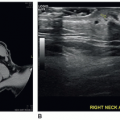
 FIGURE 23-2 Coronal sections. A: A coronal section of the hip with the leg in the neutral position shows the femoral head (H), the iliac line superiorly (i), the labrum (arrow), and the acetabulum (A). B: This coronal section in a flexed position demonstrates a similar anatomy; however, the femoral neck is not seen. |
The Ortolani maneuver is performed on a supine infant and the index and middle fingers of the examiner are placed along the greater trochanter with the thumb placed along the inner thigh. The hip is flexed to 90 degrees and held in a neutral position as the hip is gently abducted, simultaneously lifting the leg anteriorly. A palpable physical movement called a clunk is felt as the dislocated femoral head reduces into the acetabulum.8,9
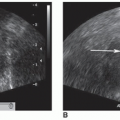
 FIGURE 23-3 Ossification. The femoral head ossification is seen on a 5-month-old female. |
Visual Assessment
Other features that arouse suspicion include asymmetry of thigh folds, a positive Allis or Galeazzi sign, and discrepancy of leg lengths. These physical findings alert the examiner that abnormal relationships of the femoral head to the acetabulum (dislocation and subluxation) may be present.
A visual assessment should be performed for signs that would raise suspicion of DDH. Dislocation can be observed using the Allis or Galeazzi sign of the relative shortness of the femur by noting that when the knees are flexed, one knee will appear lower than the other. For unilateral hip dysplasia, the Allis or Galeazzi sign can be assessed with the patient in the supine position with the knees flexed, noting limb-length discrepancy. Other visual signs include a shortening of the thigh, redundant and asymmetric skin folds on the thigh of the affected leg, and asymmetry of gluteal folds.2,8,9 A female profile with an increased pelvic width and the appearance of a waist may also be noted. A positive clinical examination may prompt a follow-up sonographic examination. To reduce the likelihood of a false-positive examination owing to laxity of the muscles in response to maternal hormones, sonographic examination of the hip should be performed between 4 and 6 weeks of age.10 In a toddler, DDH may present as an abnormal gait.2
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


