The Mammography Report and the Medical Audit
THE MAMMOGRAPHY REPORT
The mammographic report should be concise, accurate, and directive. For screening exams, a report with pertinent negatives is used for normal studies, and a report stating there is a mass, distortion, or calcifications requiring further evaluation is issued for potentially abnormal studies. Description and characterization of findings are relegated to the diagnostic setting. Time and time again, we find that the information available to us on the screening study is limited and may actually be misleading. In our opinion, trying to make definitive statements on a screening study is not optimal. As discussed in Chapter 2, the only assessment categories we use for screening studies are as follows: 1, negative; 2, benign; and 0, incomplete, requiring additional imaging evaluation.
For a diagnostic exam after a screening study, we need to determine whether there is a lesion and, if there is, to characterize it and make a decision about the next appropriate step. For a diagnostic exam in a patient presenting with a sign or symptom related to the breast, we need to correlate imaging findings (if any) with the area of clinical concern. This may require one or two mammographic images or an ultrasound and, in some patients, imaging-guided needle biopsy. The bottom line: Is there a finding that may represent breast cancer? What is the next step? Return to screen? Short-interval follow-up because the lesion is probably benign? Or biopsy? On these studies, all assessment categories are used, although category 0 is not typically used.
Before dictating a report, review films with comparisons (if available), make a decision about what you think is going on, and provide an appropriate recommendation and direction. Focus immediately on the relevant observations. Do not use the report to make up your mind as you go along, describing every inconsequential (“ditzel”) and benign finding. If you do not have enough information to make up your mind, then do whatever you need to do to get the information. On clinically occult lesions, the radiologist interpreting the mammogram should provide guidance and a final recommendation.
Work hard at making your mammography reports concise, accurate, and directive. After complete imaging workups, make up your mind about the significance of any findings.
Read your reports. Do they make sense? Are they logical, or do you jump from one finding to the next or from one breast to the other? Make every effort to issue reports that are helpful to the clinician. Eliminate excessive verbiage that is often confusing and can
be misleading. Be precise; instead of saying a mass is small or large, give a measurement. The description of the findings belongs in the body of the report, and the impression should be your decision with a recommendation that is supported and justified by the findings of your workup. The impression should not be a repetition of the findings.
be misleading. Be precise; instead of saying a mass is small or large, give a measurement. The description of the findings belongs in the body of the report, and the impression should be your decision with a recommendation that is supported and justified by the findings of your workup. The impression should not be a repetition of the findings.
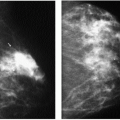
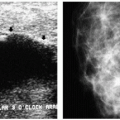
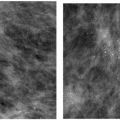
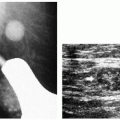
The “probably benign” category is used in the diagnostic setting. We do not use this category on screening studies because characterization of the lesion is required to justify this designation (4, 5, 6, 7, 8, 9). Masses that appear well circumscribed on screening studies may have small spiculations and irregular margins on spot compression and spot compression magnification views. Ultrasound is undertaken because if the mass is a simple cyst, short-interval follow-up is not appropriate. Calcifications that appear benign on screening studies may have pleomorphic features on magnification views, and some that appear linear and of concern are identified as benign with additional evaluation. Finally, some of the lesions are characterized as benign after additional images or ultrasound, and short-interval follow-up is not indicated.
This category should not be used to circumvent complete mammographic workups or decision making. It is probably a designation that is only appropriate in women with no prior studies. If the lesion is present on prior studies with no interval change or a decrease in size, a short-interval follow-up adds no additional information. If the lesion has increased in size compared with prior studies and is solid on ultrasound, a biopsy is indicated (not short-interval follow-up).
Usually, short-interval follow-up refers to one extra study of the affected breast 6 months after the initial study. Rarely, when considering an inflammatory, postsurgical, or traumatic etiology for a finding, is anthing less than 6 months appropriate. The probably benign lesions and the data in support of follow-up are defined for mammographic findings (not ultrasound findings) and include localized or multiple findings (4, 5, 6, 7, 8, 9). Included among the localized findings are nonpalpable, noncalcified, solid, round or oval, predominantly well-circumscribed masses, irrespective of the size of the mass or age of the patient; nonpalpable, focal asymmetry with concave margins and interspersed fat; an asymptomatic, single, dilated duct; and a cluster of small, round or oval calcifications. Included among the multiple findings are multiple (three or more) similar findings, distributed randomly and often bilaterally: circumscribed masses and round or oval, small calcifications in tight clusters (or scattered individually throughout the breast).
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


