2 The normal hepato-biliary system
Introduction
Familiarity with normal anatomy, and technical expertise in comprehensively examining an organ are essential. The latter can be obtained only by practice in a clinical environment under proper supervision. Having comprehensive medical and anatomical knowledge is necessary, but it does not enable you to scan, any more than being an air traffic controller enables you to fly an airliner (Box 2.1).
Box 2.1
It is good practice, particularly on the patient’s first attendance, to scan the whole of the upper abdomen, focusing particularly on the relevant areas, but also excluding or identifying any other significant pathology. A full abdominal survey would usually include the liver, gallbladder, biliary tree, pancreas, spleen, kidneys and retroperitoneal structures.1 Apart from the fact that many pathological processes can affect multiple organs, a number of significant (but clinically occult) pathological processes are discovered incidentally, for example renal carcinoma or aortic aneurysm. A thorough knowledge of anatomy is assumed at this stage, but diagrams of upper abdominal sectional anatomy are included in the appendices to this chapter for quick reference (see Chapter 2 Appendices, pages 47–50.)
General pointers on upper abdominal technique
The liver
Normal appearances
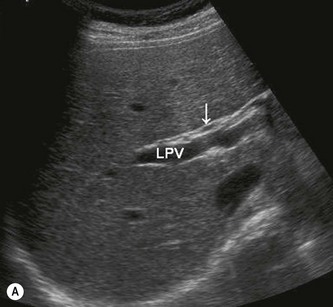
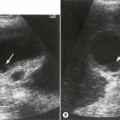
The liver is a homogeneous, mid-grey organ on ultrasound. It has the same, or slightly increased echogenicity when compared to the cortex of the right kidney. Its outline is smooth, the inferior margin coming to a point anteriorly (Fig. 2.1). The liver is surrounded by a thin, hyperechoic capsule, which is difficult to see on ultrasound unless outlined by fluid (Fig. 2.2).


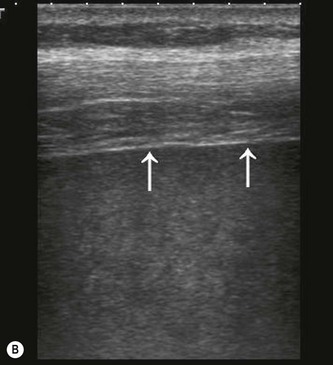
Fig. 2.2 • (A) The capsule of the liver is a thin, hyperechoic layer seen anteriorly.
(B) It is much better appreciated at higher frequencies (arrows) (7.5 MHz).
The smooth parenchyma is interrupted by vessels (see below) and ligaments (Figs 2.3–2.15), and the liver itself provides an excellent acoustic window onto the various organs and great vessels situated in the upper abdomen.
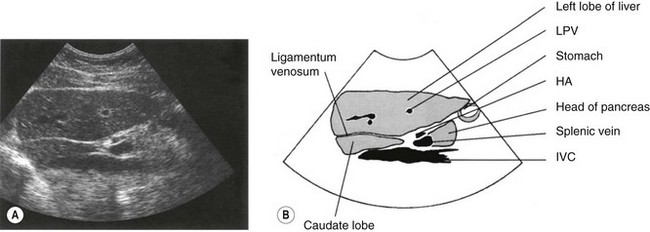
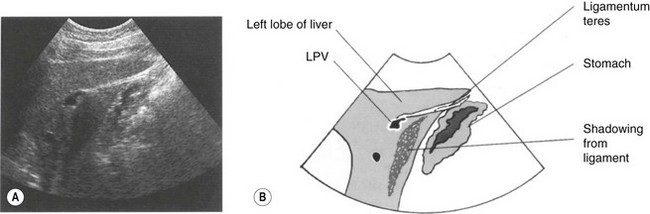
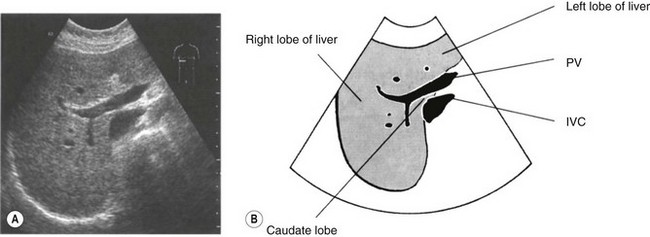
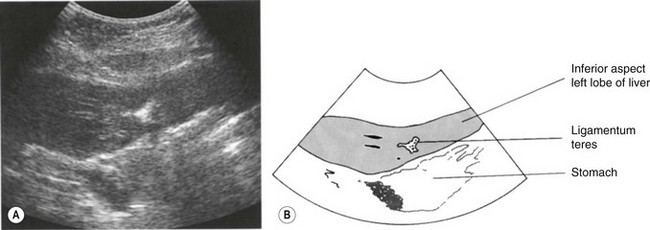
The ligaments are hyperechoic, linear structures; the falciform ligament, which separates the anatomical left and right lobes, is situated at the superior margin of the liver and is best demonstrated when surrounded by ascitic fluid. It surrounds the left main portal vein (PV) and is known as the ligamentum teres as it descends towards the infero-anterior aspect of the liver (Figs 2.9, 2.15). The ligamentum venosum separates the caudate lobe from the rest of the liver (Fig. 2.6).
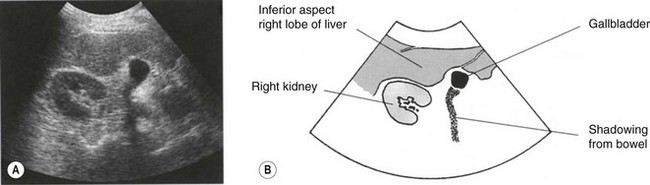
The size of the liver is difficult to quantify, as there is such a large variation in shape between normal subjects and direct measurements are notoriously inaccurate. Size is therefore usually assessed subjectively. Look particularly at the inferior margin of the right lobe which should come to a point anterior to the lower pole of the right kidney (Fig. 2.1). A relatively common variant of this is the Reidel’s lobe, an inferior elongation of segment V1 on the right. This is an extension of the right lobe over the lower pole of the kidney, with a rounded margin (Fig. 2.16), and is worth remembering as possible cause of a palpable right upper quadrant ‘mass’.
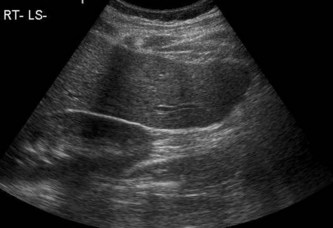
Fig. 2.16 • LS through the right lobe, demonstrating a Reidel’s lobe extending below the right kidney. (Compare with the normal liver in Figure 2.1).
The segments of the liver
The segmental anatomy system, proposed by Couinaud in 1900,2 divides the liver into eight segments, numbered in a clockwise direction. They are divided by the portal and hepatic veins and the system is used by surgeons today when planning surgical procedures (Fig. 2.17). This system is also used when localizing lesions with CT and MRI.
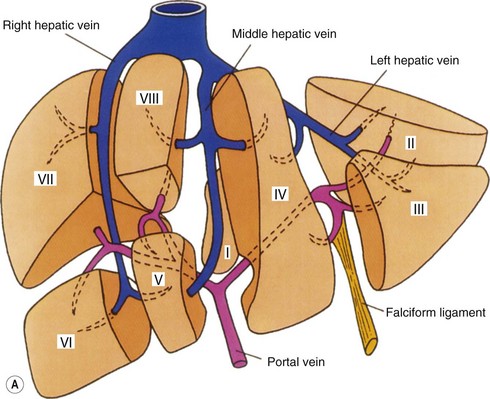


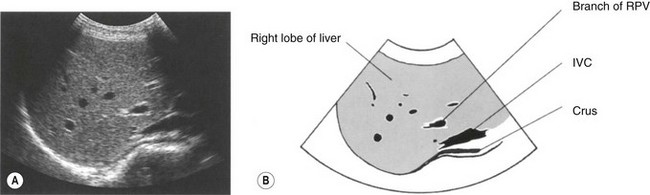
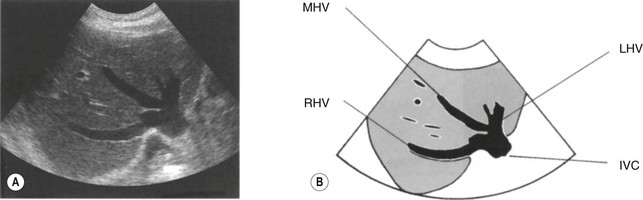
Identifying the different segments on ultrasound requires the operator to form a mental three-dimensional (3D) image of the liver. The dynamic nature of ultrasound, together with the variation in planes of scan, make this more difficult to do than for CT or MRI. However, segmental localization of hepatic lesions by an experienced operator can be as accurate with ultrasound as with MRI.3 Systematic scanning through the liver, in transverse section, identifies the main landmarks of the hepatic veins (Fig. 2.11) separating segments VII, VIII, IV and II in the superior part of the liver. As the transducer is moved inferiorly, the portal vein appears, below which segments V and VI are located.
Hepatic vasculature
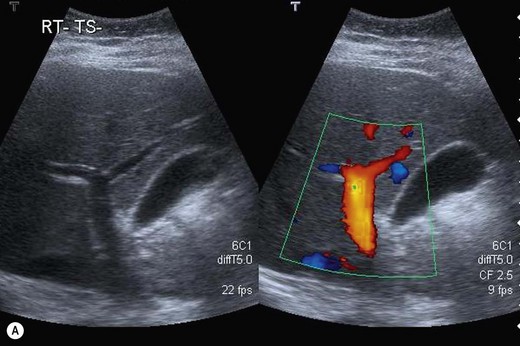
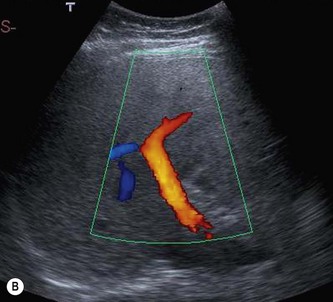
The portal veins radiate from the porta hepatis, where the main portal vein (MPV) enters the liver (Fig. 2.18). The veins are encased by the hyperechoic, fibrous walls of the portal tracts, which make them stand out from the rest of the parenchyma. Also contained in the portal tracts are a branch of the hepatic artery (HA) and a biliary duct radicle. These latter vessels are too small to detect by ultrasound in the peripheral parts of the liver, but can readily be demonstrated in the larger, proximal branches (Fig. 2.19).
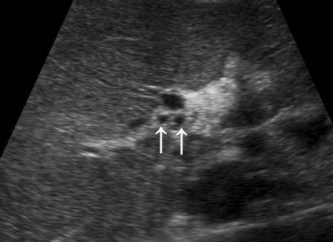
At the porta, the hepatic artery generally crosses the anterior aspect of the portal vein, with the common duct anterior to this (Fig. 2.20). In a common variation the artery lies anterior to the duct. Peripherally, the relationship between the vessels in the portal tracts is variable (Fig. 2.21).



The three main hepatic veins, left (LHV), middle (MHV) and right (RHV), can be traced into the IVC at the superior margin of the liver (Fig. 2.11





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


