Stage
Criteria
0
Normal or nondiagnostic radiograph, bone scan, and MRI
I
Normal radiograph; abnormal bone scan and/or MRI
A – Mild
(<15 % of head affected)
B – Moderate
(15–30 %)
C – Severe
(>30 %)
II
Lucent and sclerotic changes in femoral head
A – Mild
(<15 %)
B – Moderate
(15–30 %)
C – Severe
(>30 %)
III
Subchondral collapse (crescent sign) without flattening
A – Mild
(<15 % of articular surface)
B – Moderate
(15–30 %)
C – Severe
(>30 %)
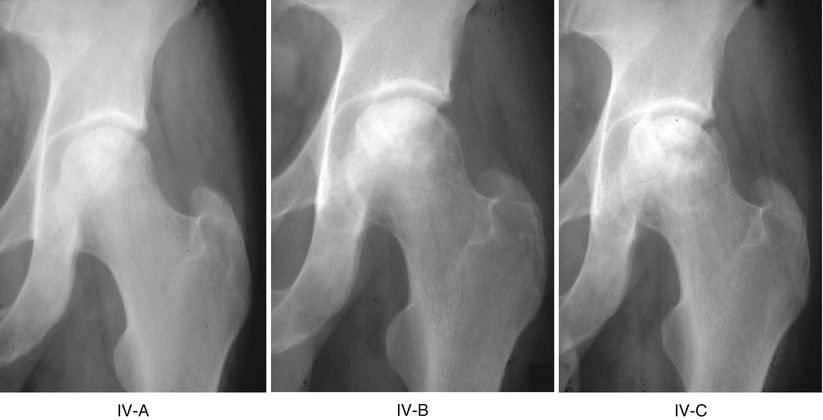
IV
Flattening of femoral head
A – Mild
(<15 % of surface and <2 mm depression)
B – Moderate
(15–30 % of surface or 2–4 mm depression)
C – Severe
(>30 % of surface or >4 mm depression)
V
Joint narrowing and/or acetabular changes
A – Mild
B – Moderate
C – Severe
Average of femoral head involvement, as determined in stage IV, and estimated acetabular involvement
VI
Advanced degenerative changes
25.1.1 Determining Stage
Stage 0. Stage 0 indicates that a hip is suspected of having ON although radiographs and MR are normal or nondiagnostic, such as a painful hip in a patient with proven ON in the opposite hip. Stage 0 would include hips evaluated too soon after a precipitating event for changes to appear or hips with too small an area of involvement to be detected with current modalities. The diagnosis might be made some time after the original evaluation when the lesion appears on imaging studies. A definitive diagnosis in stage 0 will also most likely be possible in the future with further refinements in our diagnostic techniques. Thus, inclusion of stage 0 will extend the useful life of this classification.
Stage I. Plain radiographs are normal, but MRI and/or technetium scans indicate the presence of ON.
Stage II. Radiographs now show definitive abnormalities consistent with ON. These consist of radiolucent and/or sclerotic regions, at times demarcated from normal bone by a sclerotic border. Rarely, the earliest radiographic findings will include generalized osteopenia of the femoral head.
Stage III. Stage III is diagnosed by the appearance of a radiolucent crescent line just beneath the subchondral end plate, but without flattening of the femoral head. This indicates collapse of the cancellous trabeculae beneath an intact articular surface. A crescent sign does not always appear as the head progresses from earlier to later stages and may be seen in only one radiographic projection. A relatively small percentage of hips will fit the criteria for stage III. However, we feel that they should be assigned a separate stage rather than being grouped together with hips which show gross flattening of the articular surface because clinical experience documents a better outcome for hips in stage III than for hips in stage IV, where flattening is already present [1, 15–18]. The hip is still spherical at this stage and it is theoretically possible to preserve its normal anatomy by bone grafting or other procedures.
Stage IV. There is now definite flattening of the femoral head which appears in either the AP, lateral, or both views. Occasionally small areas of collapse cannot be seen on plain radiographs but can be detected with CT. The acetabulum appears radiographically normal at this stage. However, early changes in the acetabular cartilage have been identified in the majority of stage IV hip patients whose pain and disability were sufficient for them to require arthroplasty. Stage IV has serious implications, because irreversible changes have taken place and a “normal” femoral head cannot be anticipated despite appropriate treatment.
Stage V. In addition to flattening of the femoral head, there is now clear radiographic evidence of joint line narrowing and later sclerosis and cystic changes in the acetabulum. Progressive degenerative changes follow.
Stage VI. Degenerative changes in both the femoral head and acetabulum have progressed to the point where the joint line is virtually obliterated and marked deformity appears. Other staging systems have grouped stages V and VI together; however, a small but definite number of hips develop changes so advanced that they can be distinguished from stage V. We thus feel that they deserve a separate designation and this allows us to follow progression more accurately.
25.1.2 Determining Extent of Involvement
After the type of radiographic and pathologic changes has determined the stage, the extent of involvement is next estimated or measured. For clinical purposes it is adequate to make a simple estimate and to describe this as mild (A), moderate (B), or severe (C). However, for research purposes it is preferable to make actual measurements as described below. No attempt is made to quantify the extent of involvement in stages 0 or VI.
In stages I and II the three-dimensional size or volume of the necrotic lesion is determined and expressed as a percentage of the entire head. In stage I this is estimated or calculated from serial MRI sections. In stage II, the MRI can be used in a similar fashion if it is available. However, in many cases where the lesion is clearly seen on radiographs, MRI will not be available and several methods can be used to determine the lesion size from plain radiographs. The most accurate involve the use of computerized image analysis. However, a reasonable estimate of lesion size has been made by some investigators using different types of angular measurements or by a simple visual estimate [1, 2, 6, 19–23].
In stage III it is first determined whether the crescent sign is more prominent in the AP or the lateral view. This view is then used to measure the length of the crescent and to express it as a percent of the length of the entire articular surface of the femoral head. This can be done with modern imaging techniques. If not available, one can use a map reading planimeter, a specially designed grid, or simple angular measurements.
In stage IV, as in stage III, measurements are made on either the AP or the lateral film, whichever shows the greatest amount of collapse. The normal contour of the femoral head before collapse is reconstituted, and then the length of the collapsed segment is measured and expressed as a percentage of the entire articular surface. The maximum depression of the collapsed segment is also measured and expressed in millimeters. This can be done as described for stage III.
In stage V the length of the collapsed segment and the amount of collapse of the femoral head are determined as described above. The degree of acetabular involvement is then estimated. The average of the femoral head and acetabular involvement determines the overall grade.
More detailed information about the University of Pennsylvania Classification can be found in our earlier publications [13, 14, 21]. These include a specific description of the methods originally used to measure lesion size and the extent of joint involvement. However, a number of technological advances using image analysis software have been made since that time, making it simpler and more accurate to obtain these measurements [22, 24].
25.2 Evaluation and Comparison with Other Classifications
The two most important features of the University of Pennsylvania Classification are the incorporation of MRI and specific measurements of lesion size as integral parts of the system. Both of these are now recognized as essential for inclusion in any effective classification. MRI is the single best modality for the early diagnosis of ON, before changes appear on radiographs. Its sensitivity and specificity have been confirmed [1, 10–12, 22–25]. Its use has made invasive mechanism for diagnosis, scintigraphy, and CT no longer necessary.
It is well established that the prognosis and hence the treatment of hips with ON is directly related to the size of the necrotic region even within the same stage [1, 15, 17–20, 22, 23, 26]. It is therefore essential to include an accurate measurement of lesion size as an integral part of the classification. This allows us to establish a prognosis, follow progression or resolution, compare different methods of treatment, and determine the best management for a patient with osteonecrosis. These represent significant improvements over older methods of classification which indicated only the stage and not the extent of involvement (Fig. 25.1).
 Ischemia and Reperfusion Injury in Bone
Ischemia and Reperfusion Injury in Bone
 Glucocorticoids (as an Etiologic Factor)
Glucocorticoids (as an Etiologic Factor)
 Alumina Ceramic-on-Highly Cross-Linked Polyethylene Bearing in Cementless Total Hip Arthroplasty in Young Patients with Osteonecrosis of Femoral Head
Alumina Ceramic-on-Highly Cross-Linked Polyethylene Bearing in Cementless Total Hip Arthroplasty in Young Patients with Osteonecrosis of Femoral Head
 Impaction Bone Grafting
Impaction Bone Grafting
 Causes of Pain in Early and Advanced Stage Osteonecrosis
Causes of Pain in Early and Advanced Stage Osteonecrosis
 Kienböck’s Disease of the Lunate
Kienböck’s Disease of the Lunate




Related posts:
Ischemia and Reperfusion Injury in Bone
Glucocorticoids (as an Etiologic Factor)
Alumina Ceramic-on-Highly Cross-Linked Polyethylene Bearing in Cementless Total Hip Arthroplasty in Young Patients with Osteonecrosis of Femoral Head
Impaction Bone Grafting
Causes of Pain in Early and Advanced Stage Osteonecrosis
Kienböck’s Disease of the Lunate
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
