Liver lesions that can be thermally ablated are classified into primary liver lesions (hepatocellular carcinoma [HCC]) and secondary liver lesions (metastases).
Percutaneous thermal ablation increases the possibility of curative treatment in patients with liver recurrence after hepatectomy from 17 to 26% and is preferred over repeat surgery because it is less invasive (lower procedural morbidity).
Less than five lesions, with each lesion having a maximum diameter of ≤3 cm (preferable)
Metastasis reported to be ablated:
Colorectal metastasis (most common metastasis)
20–25% of colon cancer patients have resectable disease in the liver; surgical resection is the curative modality and not percutaneous thermal ablation.
Percutaneous thermal ablation increases the possibility of curative treatment in patients with liver recurrence after hepatectomy from 17 to 26% and is preferred over repeat surgery because of its less invasiveness (lower procedural morbidity).
Local control of malignant liver disease can be intended to
Cure
Temporize and for local control while awaiting liver transplantation (for HCC only and not for liver metastasis)
Be palliative (painful metastasis stretching Glisson, capsule)
Result summary for percutaneous thermal ablation of HCC
Local tumor control (technical success): 95–100%
Progression of disease after treatment over 2 years: 2–18%
Overall 3-year survival rate is 74–80%, but depends on the underlying liver disease as well.
Result summary for percutaneous thermal ablation of colorectal metastasis
Local tumor control (technical success): 83–90%
Progression of disease after treatment: 17% (especially with tumor metastasis >3 cm in diameter)
Overall 3-year survival rate: 28–68%
Overall 5-year survival rate: 24–44%
Distant metachronous metastases occur in 35% of patients.
However, survival rates of patients undergoing percutaneous thermal ablation are similar to those of patients who undergo surgical resection with the same level of local control of metastases and probably less morbidity and mortality.
Result summary for percutaneous thermal ablation of breast metastasis
Local tumor control (technical success): >95%
Progression of disease with development of new metastasis occurs in up to 58% of patients.
Alternatives
There is no firm evidence to establish the optimal first-line treatment of early stage HCC because of lack of randomized controlled trials.
To refuse the percutaneous ablation or any other therapy
Surgery (hepatic resection)
Treatment of choice for noncirrhotic patients with HCC (5% of HCC patients)
Procedure-related mortality: <1–3%
Overall 5-year survival rate (with good quality care): >70%
5-year survival rate in patients with portal hypertension: 50%
5-year survival rate in patients with portal hypertension and high bilirubin: 30%
Liver transplantation
Best treatment for patients with solitary lesion <5 cm or early multifocal lesions, providing that there are ≤three lesions and all <3 cm in diameter
Only option that provides potential cure for both HCC and the underlying liver disease
Local control of tumor while awaiting liver transplantation can be achieved utilizing percutaneous thermal ablation techniques.
Laparoscopic-guided thermal ablation
Applicable to superficial lesions that can be identified and are accessible laparoscopically
Ability to displace/remove bowel away from the target lesion
Advantages of percutaneous thermal ablation
Can be performed on nonsurgical candidates
Can be performed on postoperative patients
Repeatability of treatment if initial treatments are incomplete
Can be used with regional and systemic chemotherapy
Minimally invasive
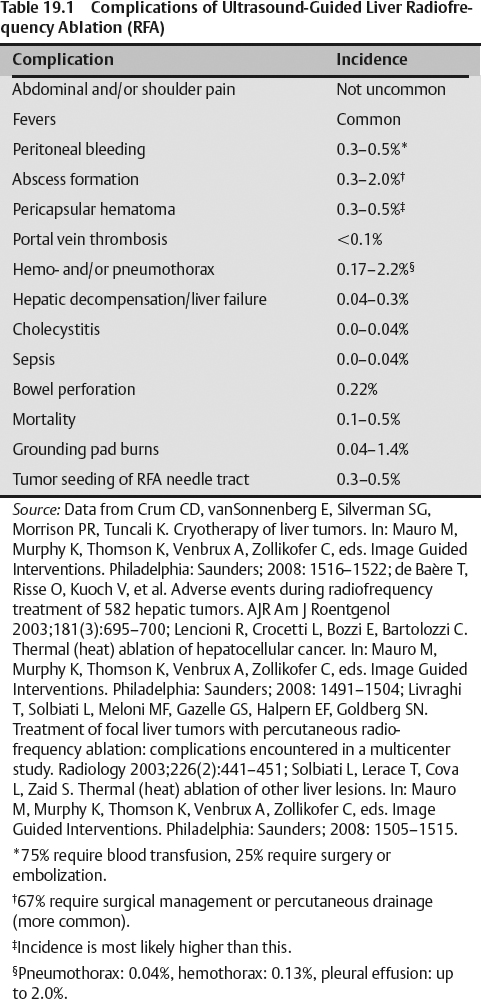
Limited complications
Usually preserves hepatic function
Limited hospital stay/outpatient
Limited procedural cost
Can be performed on nonsurgical candidates or postoperative cases
The following are summaries of types of probes. Details of the probes’ biomedical engineering are beyond the scope of this book.
Radiofrequency ablation (RFA) systems
The radiofrequency generator and the patient are the main components of an electric circuit.
The generator is the source of the alternating current and the patient’s body is the resistor.
The resistance in the tissue (impedance) to the radiofrequency current is what generates heat and creates a thermal ablation effect.
The thermal ablative (radiofrequency) electrode enters the body and alternating electric current passes directly into the body. However, a return connection to the generator is required. This return is established by grounding pads usually placed on the patient’s thighs.
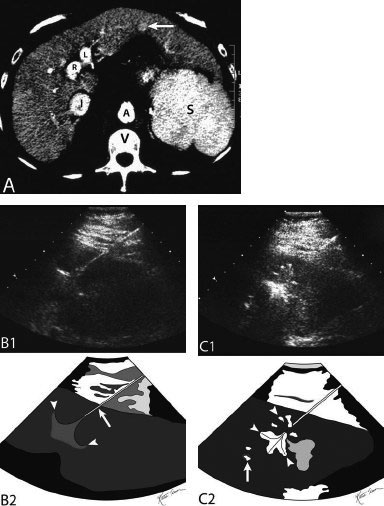
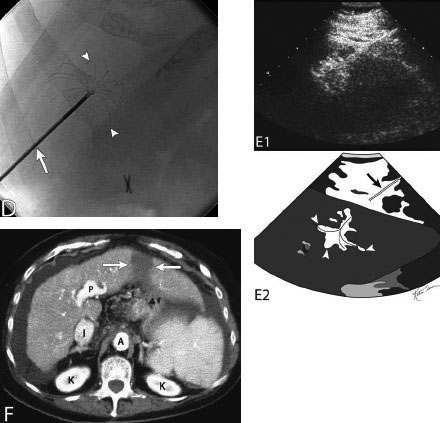
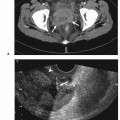
Fig. 19.1 Left lateral segment ultrasound-guided radiofrequency ablation. (A) Contrast-enhanced axial computed tomography (CT) image at the level of the aortic hiatus. An enhancing lesion is seen in the left lateral segment (arrow) (R, right portal vein; L, Left portal vein; I, Inferior vena cava [IVC]; A, aorta; V, vertebra; S, spleen). (B) Gray-scale ultrasound image (top) and schematic sketch (bottom) of the left hepatic lobe after the operator has advanced the radiofrequency probe (arrow) and after deploying the tines (arrowheads). (C) Gray-scale ultrasound image (top) and schematic sketch (bottom) of the left hepatic lobe during radiofrequency ablation. Due to cavitation, there is increased echogenicity around the probe/tines (arrowheads). The arrow points to air in an adjacent vessel (bile duct/portal vein). (D) Fluoroscopic image during the radiofrequency ablation of the lesion in Fig. 19.1A. The tines are seen deployed (arrowheads) through the probe shaft (arrow). Fluoroscopy is used to redeploy the LeVeen probe when performing radiofrequency ablation at multiple stations. (E) Gray-scale ultrasound image (top) and schematic sketch (bottom) of the left hepatic lobe after radiofrequency ablation. Due to cavitation there is increased echogenicity around the probe/tines (arrowheads). Still noted is the probe shaft (arrow). To remove the probe, the tines are retracted and the probe is removed. (F)
Only gold members can continue reading. Log In or Register to continue