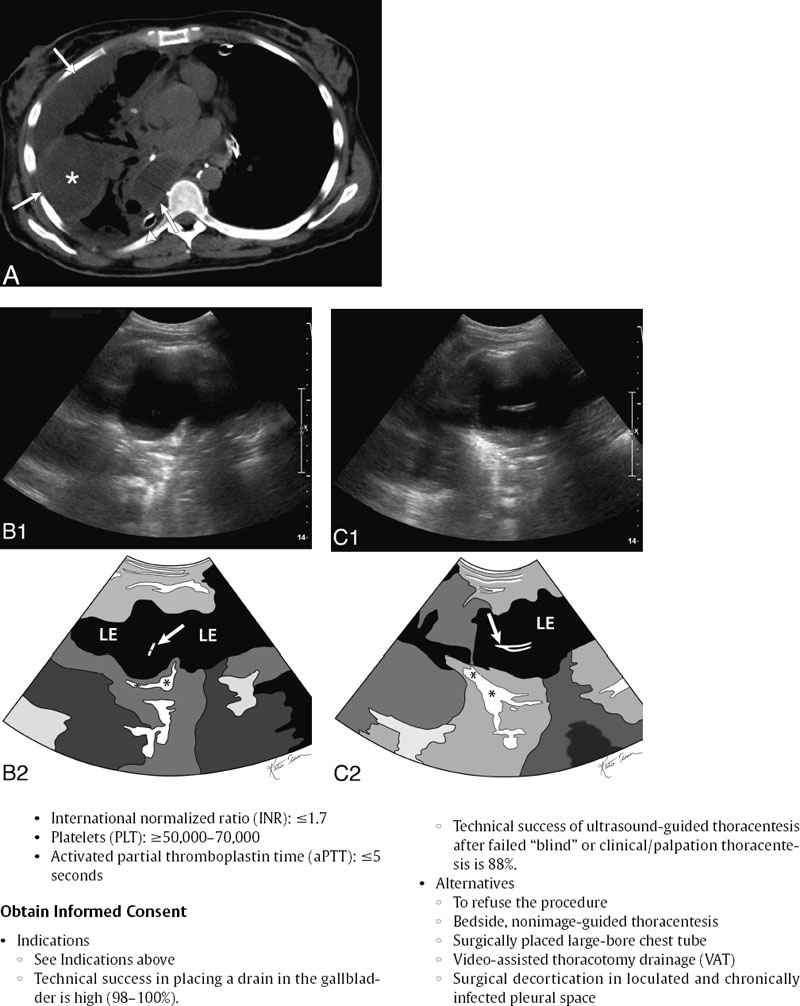
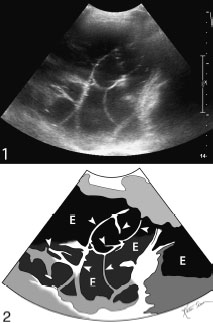
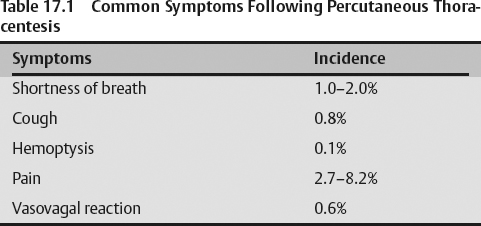
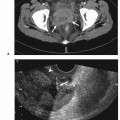
17 Thoracentesis Fig. 17.1 Drainage of postoperative infected pleural space (empyema). (A) Unenhanced axial computed tomography (CT) image of the lower chest in a patient status postthoracic surgery demonstrated thick-walled loculated collections (arrows) in the pleural space. One of these locules has a thick wall (asterisk in center of it). A large-bore surgically placed chest tube is seen in the chest bases, posteriorly (arrowhead). (B) Gray-scale ultrasound image of the fluid collection in Fig. 17.1A (top) and schematic sketch of it (bottom). A 21-gauge needle has been advanced into the pleural collection (arrow). The underlying lung is seen (asterisk) (LE, loculated pleural effusion). (C) Gray-scale ultrasound image of the fluid collection in (top) and schematic sketch of it (bottom). A 10-French drain (arrow) is now seen in the target pleural collection (LE, locu-lated pleural effusion). The underlying lung is seen (asterisk). Fig. 17.2 Gray-scale ultrasound image of a septated pleural effusion (top) and schematic sketch of it (bottom). Numerous septa are seen (arrowheads) crisscrossing the pleural effusion (E).
Indications
By Presentation
By Etiology/Fluid Type
Contraindications
Relative Contraindication
Preprocedural Evaluation
Evaluate Prior Cross-Sectional Imaging
Evaluate Preprocedure Laboratory Values
Obtain Informed Consent
Equipment
Ultrasound Guidance
Standard Surgical Preparation and Draping
Local Infiltrative Analgesia Administration
Sharp Access Devices
Tubular Access Devices
Suction/Water Seal Devices
Technique
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


