and Filiz Özülker1
(1)
Nuclear Medicine, Okmeydani Training and Research Hospital, Istanbul, Turkey
4.1 Case 1: Thyroid Incidentaloma Identified by 18F-FDG PET/CT
History
A 42-year-old man had the surveillance FDG PET/CT scan because of history of a malignant melanoma.
Findings
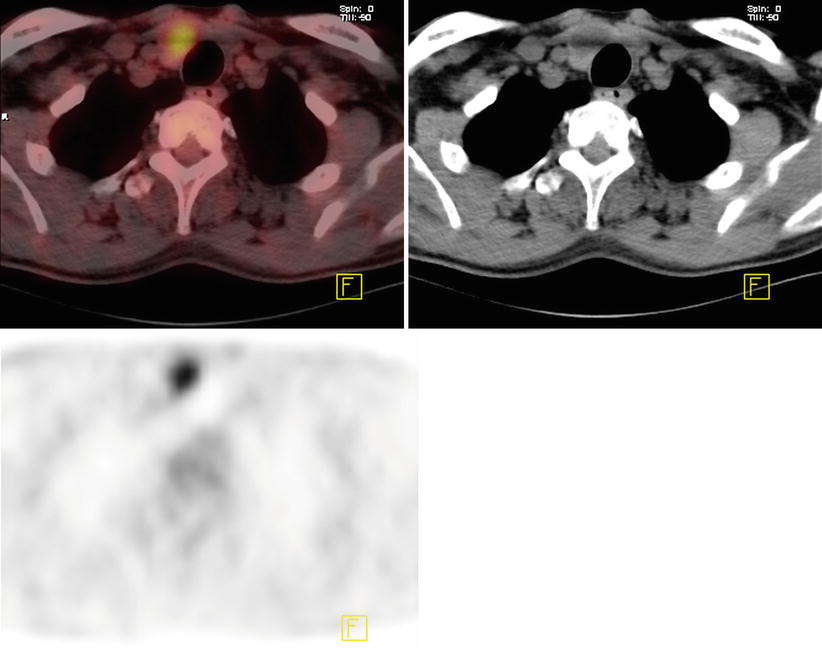
Fig. 4.1
Hypermetabolic thyroid nodule at right lobe of thyroid gland with an SUVmax 7
Interpretation
Hypermetabolism at the right thyroid lobe is suspicious for malignancy.
Outcome
FNA of the hypermetabolic nodule at right thyroid lobe revealed papillary thyroid carcinoma.
Teaching Point
The prevalence of focal thyroid lesions on FDG PET/CT is 1.2–4.0 %. Of the thyroid incidentalomas that underwent FNA and surgery, 14–47 % were found to be malignant.
4.2 Case 2: 18F-FDG PET CT Performed for Evaluation of Thyroid Nodule
History
A 38-year-old female was found to have a rapidly growing single nodule on USG measuring 1.5 × 1.9 × 1.3 cm and having microcalcifications in it. The nodule was hypoactive on thyroid scintigraphy and the thyroid function tests of the patient was normal. After an indeterminate fine needle aspiration biopsy, the patient underwent 18F-FDG PET CT scan for determination of the malignant nature of the nodule.
Findings
Fig. 4.2
Axial PET and CT images show intensely hypermetabolic thyroid nodule at left lobe of thyroid gland (SUVmax 33)

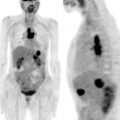
Fig. 4.3
MIP image
Interpretation
The nodule showing high FDG uptake at the left thyroid lobe is suspicious for malignancy.
Result
The patient underwent left lobectomy and isthmectomy and histopathology turned out to be papillary thyroid cancer.
Teaching Point
18F-FDG PET CT showed a high sensitivity in detecting malignancy in patients with indeterminate FNAB results. In a meta-analysis, 18F-FDG PET or PET/CT correctly detected malignant lesions, with a very high pooled sensitivity of 89.0 %. The malignant nodules with a dimension >1–1.5 cm rarely become negative on FDG PET.
4.3 Case 3: Staging of Insular Thyroid Carcinoma
History
A 88-year-old female who was diagnosed with poorly differentiated thyroid carcinoma underwent 18F-FDG PET/CT study.
Findings
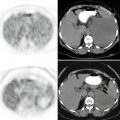
Fig. 4.4
Axial CT and fusion images of PET/CT show intensely hypermetabolic lesion with irregular borders and hypometabolic necrotic center at thyroid gland (a, b)
Fig. 4.5
Axial CT and fusion images show intensely hypermetabolic lytic lesion at right ischium (a, b)
Fig. 4.6
Axial images show multiple lung nodules showing increased FDG uptake and hypermetabolic activity at the lytic lesion at right posterior elements of D6 vertebra (a–d)
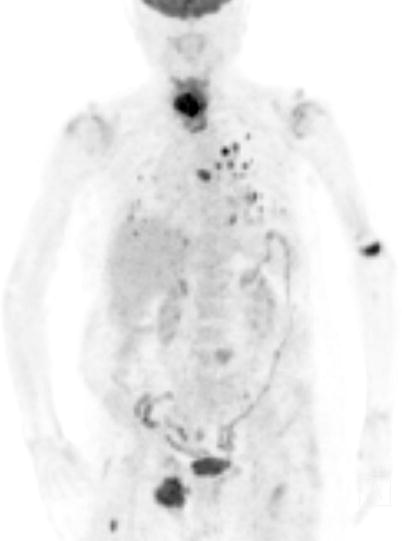
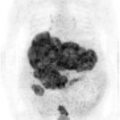
Fig. 4.7
MIP image shows additional pathologically increased FDG uptake sites at distal diaphysis of left humerus, left side of corpus of L4 vertebra, and proximal right femur diaphysis
Interpretation
FDG avid primary malignancy at thyroid gland and multiple metastases at lung parenchyme and bony structures
Teaching Point
Well differentiated thyroid carcinoma shows poor FDG uptake and high I-131 uptake, whereas more malignant types (PDTC) appear to retain FDG more avidly while their I-131 uptake is low. This flip-flop phenomenon is attributed to the characterization of progressive dedifferentiation of thyroid tumors by upregulation of glucose transporters (GLUT1) and reduction of expression of sodium-iodide symporter (NIS).
18F-FDG PET/CT is currently used for initial staging and follow-up of high-risk patients with poorly differentiated thyroid cancers. It is also used as a prognostic tool in patients with metastases, for the evaluation of posttreatment response, and as selection tool in patients not eligible to radioiodine therapy.
4.4 Case 4: Restaging of Insular Thyroid Carcinoma
History
A 71-year-old female who has a history of insular thyroid carcinoma. The patient is status postthyroidectomy and I-131 ablation. He is now being evaluated for high thyroglobulin levels (500 ng/ml). The patient is referred to 18F-FDG PET/CT scan after a diagnostic whole body I-131 scan gave negative result.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


