Most commonly Roux-en-Y gastric bypass and liver transplantation
Much more common when Roux loop is placed in retrocolic position
• Almost always congenital in children
May be secondary to prenatal intestinal ischemia with thinning of mesenteric leaves
CLINICAL ISSUES
• Can occur in both adults (65%) and children (35%):
• Larger transmesenteric hernias present with symptoms of small bowel obstruction
Symptoms are more likely to be acute compared to other types of internal hernias
High risk of volvulus (∼ 30%) and ischemia (∼ 40%)
Onset usually months after original surgery
• Treatment: Laparotomy with bowel decompression and surgical correction of mesenteric defect
(Left) Axial graphic shows dilated small bowel herniating through a mesenteric defect . Note the peripheral position of the small bowel , medial displacement of the colon , and the displaced mesenteric vessels .
(Right) Axial CECT in a patient with prior colonic resection shows a cluster of dilated small bowel in the left abdomen. These loops lie ventral to the transverse colon , and the mesenteric vessels are distorted and congested. These findings are typical of a transmesenteric hernia.
(Left) Axial CECT in a patient with a history of prior abdominal surgery demonstrates multiple dilated, fecalized loops of small bowel in the left abdomen, in keeping with a small bowel obstruction.
(Right) Coronal CECT in the same patient demonstrates that these bowel loops are clustered in the lateral aspect of the abdomen, directly abutting the abdominal wall, and displacing the colon . This constellation of findings is classic for a postoperative transmesenteric hernia.
TERMINOLOGY
Synonyms
• Transmesenteric congenital hernia
Definitions
• Protrusion of bowel loops through acquired or congenital abdominal mesenteric defect
IMAGING
General Features
• Best diagnostic clue
Small bowel obstruction in patient status post liver transplant or Roux-en-Y surgery with dilated bowel loops abnormally clustered at periphery of abdomen
• Location
Abnormal opening in mesentery of small bowel or colon
– Most commonly found in right mid abdomen
Postoperative hernias from Roux-en-Y gastric bypass surgery occur in 3 primary locations
– Transverse mesocolon (80%)
– Small bowel mesentery (14%)
– Behind Roux loop (6%) (Peterson-type hernia)
Hernias after liver transplant can occur in transverse mesocolon (more common) or small bowel mesentery
• Size
Mesenteric defect varies from few mm to few cm
Radiographic Findings
• Radiography
“Closed loop” obstruction: Markedly distended segment of small bowel with multiple air-fluid levels
Crowded and dilated small bowel loops in abnormal location (often towards periphery of abdomen)
CT Findings
• Small bowel obstruction with dilated small bowel loops and discrete transition point from dilated to nondilated bowel and distally decompressed small bowel loops
• Clustered, tethered loops of small bowel in periphery of abdominal cavity immediately adjacent to abdominal wall
Bowel loops found lateral to colon unlike normal appearance, where colon is lateral to small bowel
Displacement of overlying omental fat of herniated bowel loop, with obstructed bowel loops directly contacting abdominal wall
Colon displaced posteriorly and inferiorly (most common) or medially (less common)
Right or left displacement of main mesenteric trunk with stretching and tethering of more distal mesenteric vascular branches
Most often occurs in right hemiabdomen
Hernia usually not encapsulated or enveloped in sac unlike paraduodenal hernias
• Additional findings often suggestive of closed loop obstruction or volvulus
Whirl sign (small bowel volvulus with twisting of mesenteric vessels around a central point)
Mesenteric vessels appear engorged, crowded, or twisted
Thickened bowel wall and ascites, particularly in cases with bowel ischemia
• Smaller transmesenteric hernias after Roux-en-Y gastric bypass via transverse mesocolon
Small retrogastric cluster of small bowel loops with mass effect on posterior stomach wall
– Redundant dilated Roux loop
– No colon or fat displacement
Fluoroscopic Findings
• Small bowel follow through
Crowding of bowel loops in abnormal location at periphery of abdomen (most common on right side of abdomen)
Bowel loops do not appear contained in sac or have confining border
Varying degrees of small bowel obstruction (SBO) with discrete point of transition between dilated and nondilated bowel
Some degree of fixation, stasis, and delayed flow of contrast seen in herniated bowel
Lateral films useful to demonstrate displacement of herniated bowel loops
Ultrasonographic Findings
• Grayscale ultrasound
Dilated small bowel loops in abnormal location
Angiographic Findings
• Superior mesenteric arteriogram: Abrupt angulation and displacement of visceral branches passing through mesenteric defect to herniated loops
Imaging Recommendations
• Best imaging tool
CECT
DIFFERENTIAL DIAGNOSIS
Closed Loop Bowel Obstruction
• Obstruction of small bowel at 2 points in single location forming “closed loop”
• Most often due to adhesions, but caused occasionally by internal or external hernia
• High risk of bowel infarction, strangulation, and volvulus
• Fluid-filled loops of markedly dilated small bowel with tethered, clumped configuration
Dilated bowel loops and stretched mesenteric vessels appear to radiate towards a central point
Only gold members can continue reading. Log In or Register to continue





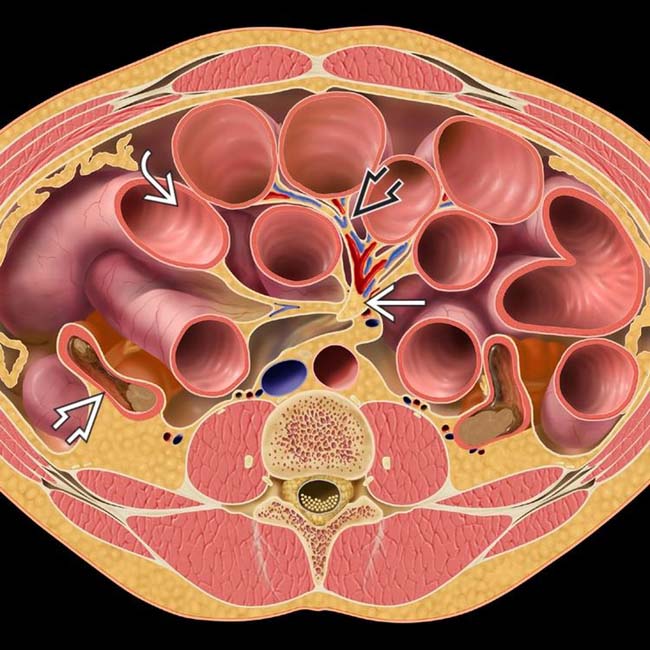
 . Note the peripheral position of the small bowel
. Note the peripheral position of the small bowel  , medial displacement of the colon
, medial displacement of the colon  , and the displaced mesenteric vessels
, and the displaced mesenteric vessels  .
.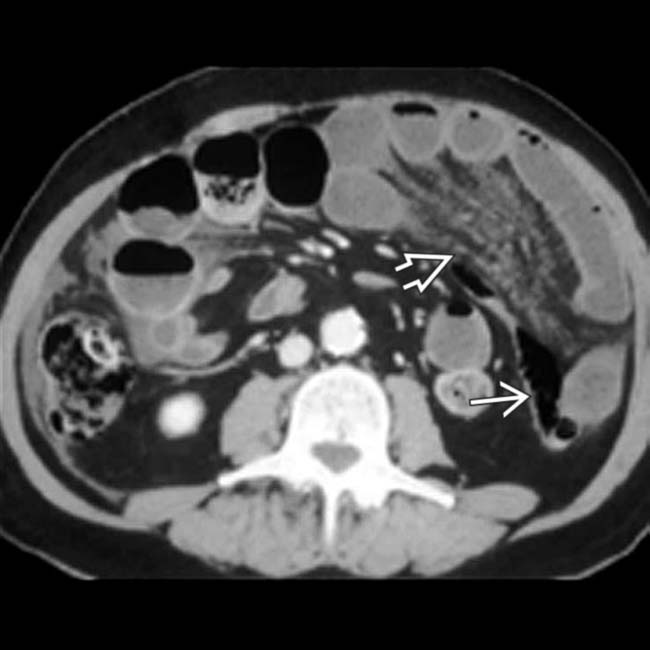
 , and the mesenteric vessels
, and the mesenteric vessels  are distorted and congested. These findings are typical of a transmesenteric hernia.
are distorted and congested. These findings are typical of a transmesenteric hernia.
 in the left abdomen, in keeping with a small bowel obstruction.
in the left abdomen, in keeping with a small bowel obstruction.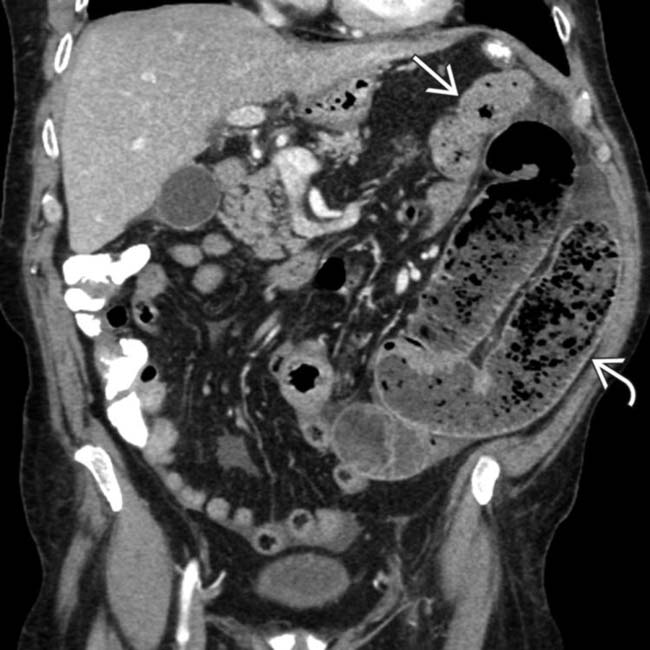
 are clustered in the lateral aspect of the abdomen, directly abutting the abdominal wall, and displacing the colon
are clustered in the lateral aspect of the abdomen, directly abutting the abdominal wall, and displacing the colon  . This constellation of findings is classic for a postoperative transmesenteric hernia.
. This constellation of findings is classic for a postoperative transmesenteric hernia.






 Displacement of overlying omental fat of herniated bowel loop, with obstructed bowel loops directly contacting abdominal wall
Displacement of overlying omental fat of herniated bowel loop, with obstructed bowel loops directly contacting abdominal wall Right or left displacement of main mesenteric trunk with stretching and tethering of more distal mesenteric vascular branches
Right or left displacement of main mesenteric trunk with stretching and tethering of more distal mesenteric vascular branches




















