Fig. 47.1
Transtrochanteric curved varus osteotomy is performed between the greater and the lesser trochanters, which has a merit to prevent elevation of the greater trochanter, lateral displacement of the femoral shaft which causes gluteus medius and minimus muscle disorders, delayed union or nonunion at the site of osteotomies, and leg length discrepancy, which has been commonly observed after wedge varus osteotomies
47.2 Indication of the Curved Varus Osteotomy
This procedure is indicated in cases with a residual intact area in the lateral part of the femoral head with an intact area ratio to the acetabular weight-bearing area of 33.6 % or more in a maximum abduction position (Fig. 47.2), since patients who had more than 33.6 % of the intact articular surface of the femoral head postoperatively had been reported to have a good clinical outcome (Figs. 47.3 and 47.4) [11]. Therefore, patients who had the prospect of obtaining more than 34 % intact articular surface on preoperative AP hip radiograph in maximum abduction were indicated for this operation. To prevent adduction contracture, cases in which the hip joints could not be abducted more than 20° are not indicated.
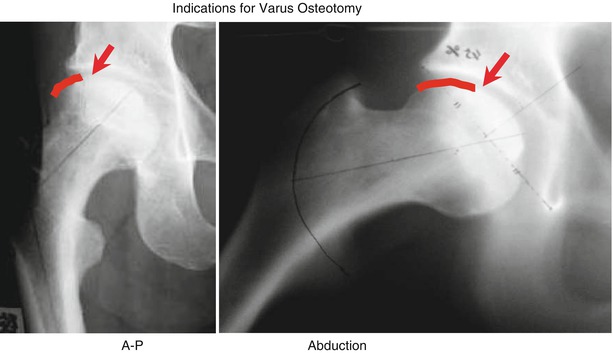
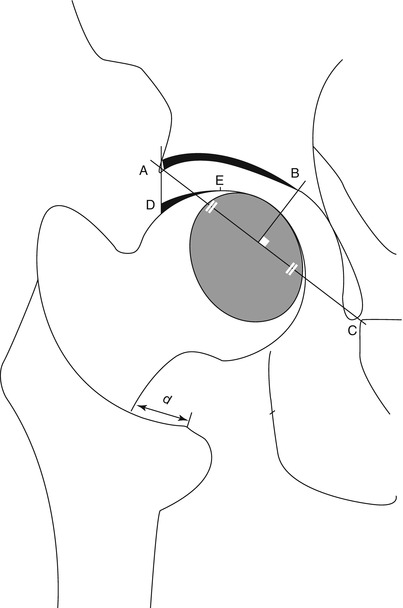
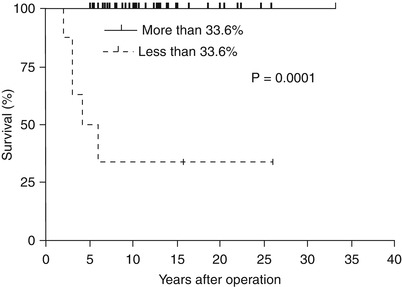
Fig. 47.2
Cases who have a residual intact area in the lateral part of the femoral head with an intact area ratio to the acetabular weight-bearing area of 33.6 % or more in a maximum abduction position (red arrow: borderline between necrotic and intact area)
Fig. 47.3
The postoperative intact area ratio of the articular surface of the femoral head to the weight-bearing area of the acetabulum on postoperative anteroposterior (AP) radiographs. Point B is determined by drawing a perpendicular line from the midpoint of A (the edge of the acetabulum) and C (the lowest point of the teardrop) to the acetabular roof. Point D represents the lateral edge of the load-bearing portion. Point E represents the medial edge of the intact articular surface of the femoral head. The postoperative intact area ratio is expressed as D – E/A – B. The planned varus angle is confirmed during surgery by measuring the moving distance of proximal femur (d), which was calculated preoperatively (Reproduced with permission and copyright© of the British Society of Bone and Joint Surgery [11])
Fig. 47.4
Kaplan-Meier survival curve shows the radiological survival rate based on the postoperative intact area ratio of 33.6 %. The endpoint is the time when the progression of collapse was observed (Reproduced with permission and copyright© of the British Society of Bone and Joint Surgery [11])
47.3 Operative Procedures
47.3.1 Operative Position
Osteotomy is performed in a complete lateral decubitus position. Since an image will be used during the operation, secure fixation should be achieved so as to obtain an accurate anteroposterior radiograph of the pelvis.
47.3.2 Skin Incision
A 15–20-cm lateral longitudinal incision is made from the proximal end of the greater trochanter to the distal end.
47.3.3 Expansion of the Hip
An incision is made on the deep fascia of the thigh and on the iliotibial band as well. The thin membranes or synovial capsules around the greater trochanter are incised with the lower extremities in a medial rotation position so that the intertrochanteric crest is exposed. The lesser trochanter is exposed subperiosteally, and the intertrochanteric crest is also elevated along the planned osteotomy line. During this process, care should be taken not to damage the nutrient vessels supplying the femoral head in the medial intertrochanteric crest. Since osteotomy is performed from the posterior side, forward expansion is not required.
47.3.4 Osteotomy Guide Setting
The varus osteotomy guide is posteriorly applied to the lateral intertrochanteric crest slightly distal end to the center of the lesser trochanter. Care should be taken to ensure that the central part of the guide is inserted 5 mm away from the intertrochanteric crest to be fixed with two pieces of cortex screw (Fig. 47.5). Also, the greater trochanter and its base should be sufficiently thick. The position should be reconfirmed on an image, and it should be adjusted as needed; the knee joint flexed to 90° and the lower leg parallel to the X-ray incident direction is the accurate median position (Fig. 47.6).
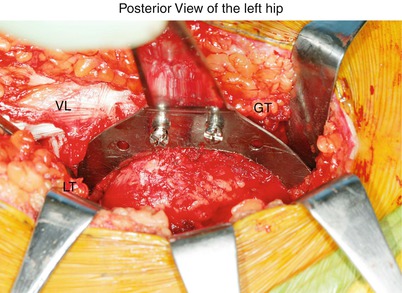

Fig. 47.5
The varus osteotomy guide is posteriorly applied to the lateral intertrochanteric crest slightly distal end to the center of the lesser trochanter. Care should be taken to ensure that the central part of the guide is inserted 5 mm away from the intertrochanteric crest to be fixed with two pieces of cortex screw. GT greater trochanter, LT lesser trochanter, VL vastus lateralis
Fig. 47.6




The guide position should be reconfirmed on an image, and it should be adjusted as needed; the knee joint flexed to 90°and the lower leg parallel to the X-ray incident direction is the accurate median position
Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
