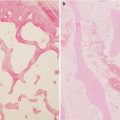
Fig. 45.1
The calculation of the combined necrotic angle from magnetic resonance imaging scans. A The angle of necrotic area in the midcoronal image. B The angle of necrotic area in the midsagittal image. The combined necrotic angle = A + B
45.3 Surgical Technique
We describe a modified surgical technique by Ha et al. [10], which uses a Y-shaped skin incision instead of the original U-shaped incision and a compression hip screw instead of cancellous screws. The Y-shaped incision enables a better exposure of the anterior capsule. Sugioka recommended fixing the osteotomy with two or three large cancellous screws. However, we have used a 120°-angled compression hip screw since 1999. The angled hip screw has several advantages compared to the cancellous screw. It prevents loss of fixation and nonunion at the osteotomy site. It also shortens the hospital stay and allows an early ambulation.
45.3.1 Surgical Pitfalls
A complete understanding of the anatomy of the medial femoral circumflex artery is of critical importance for the safe performance of this procedure.
The artery is located in the space between the quadratus femoris and obturator externus. During capsulotomy and osteotomy, extreme care should be taken not to damage this artery.
45.3.2 Patient Positioning
The patient is placed in the lateral decubitus position on a standard operating room table with the pelvis stabilized in the neutral position. Intraoperative fluoroscopy is used to confirm the appropriate osteotomy line and the position of compression hip screw (Fig. 45.2).
Fig. 45.2
The patient is placed in the lateral decubitus position and the pelvis is secured with holding devices and pads. The Y-shaped skin incision is centered at the greater trochanter. The posterior portion of the incision is started at a point that is level with the posterior superior iliac spine and along a line parallel to the posterior edge of the greater trochanter. The incision is extended distally to the center of the greater trochanter and then to a point 10–15 cm distal to the greater trochanter, in line with the femoral shaft. The anterior portion of the incision is made from the greater trochanter to the anterior superior iliac spine
45.3.3 Skin Incision
A Y-shaped skin incision is made. The posterior limb of the incision starts at the posterior superior iliac spine and proceeds to the greater trochanter and then extends to 10–15 cm distally in line with the axis of the femur. The anterior limb of the incision starts from the center of the greater trochanter to the anterior iliac spine by a length of 5–8 cm (Fig. 45.3). The length of the incision is adjusted according to the size and obesity of the patient.
Fig. 45.3
The gluteus maximus fascia is incised in line with the posterior portion of the skin incision, and the muscle fibers of the gluteus maximus are bluntly divided. Fibers of the fascia lata are divided in line with the anterior portion of the skin incision. The fat tissues covering the external rotators and the trochanteric bursa are removed to expose the sciatic nerve (arrow) along its course beneath the piriformis muscle and over the short external rotators distally
45.3.4 Fascia Incision
The fascia lata and the gluteus maximus fascia are incised in line with the skin incision. Then gluteus maximus muscle fibers are bluntly divided, giving an access to the gluteus medius and the external rotators of the hip (Fig. 45.3).
45.3.5 Exposure of the External Rotators and Sciatic Nerve
Remove the fat tissue covering the external rotators, divide the trochanteric bursa, and bluntly sweep it posteriorly to expose the sciatic nerve along its course beneath the piriformis muscle and over the short external rotators distally. The nerve is protected during the operation (Fig. 45.3).
45.3.6 Osteotomy of the Greater Trochanter
The greater trochanter is osteotomized between the gluteus medius and piriformis posteriorly and between the gluteus medius and vastus lateralis anteriorly with an oscillating saw.
45.3.7 Exposure of the Hip Joint Capsule and Capsulotomy
Expose the superior portion of the hip joint capsule by dissecting the gluteus minimus from the capsule. Expose the posterior capsule by cutting the tendons of the piriformis and obturator internus at the trochanteric insertion. Expose the inferior capsule by cutting the quadratus femoris, superior gemellus, and inferior gemellus. To avoid damage to the medial femoral circumflex artery, cut the quadratus femoris, superior gemellus, and inferior gemellus at their muscle fibers 2 cm apart from their femoral insertions. Expose the anterior capsule by developing the interval between the gluteus medius and vastus lateralis.
Once the complete exposure of the hip joint capsule is obtained, a circumferential capsulotomy is performed. The capsulotomy line should be about 1 cm apart from the acetabular rim to avoid the injury of the acetabular labrum. During the capsulotomy hold the capsule using forceps and separate it from the underlying femoral head to avoid the injury of the femoral head cartilage (Fig. 45.4).
Fig. 45.4
After the complete exposure of the hip joint capsule, the joint capsule is incised circumferentially. The capsulotomy line is 1 cm away from the acetabular rim to protect the acetabular labrum and to obtain adequate rotation of the femoral head
45.3.8 Transtrochanteric Osteotomies
Make two transtrochateric osteotomies. The first osteotomy is made about 10 mm distal to the intertrochanteric crest. The osteotomy line should be inclined at 20° from the line perpendicular to the femoral neck to place the femoral head in a varus angulation. The second osteotomy is made near the upper one-third of the lesser trochanter at 90° to the first osteotomy line (Fig. 45.5).
Fig. 45.5
The two osteotomy lines are marked with a broad straight osteotome (a), and the osteotomy is performed with the use of a reciprocating saw (b)
45.3.9 Rotation of the Proximal Segment
The proximal fragment is rotated anteriorly by 90° with a care to avoid excessive stretching or damage of the medial femoral circumflex vessels (Fig. 45.6).