A. Pivot shift
B. Hyperextension
C. Clipping
D. Dashboard
2 Which of the following correctly matches the extensor tendon with its appropriate dorsal wrist compartment?
A. Extensor pollicis longus—compartment I
B. Abductor pollicis longus—compartment II
C. Extensor indicis—compartment III
D. Extensor carpi ulnaris—compartment IV
E. Extensor digiti minimi—compartment V
3 In the setting of the following injury, what is the next most appropriate imaging study?

A. Stress radiographs of the ankle
B. Tibia/fibula radiographs
C. Ankle MRI
D. Ankle CT
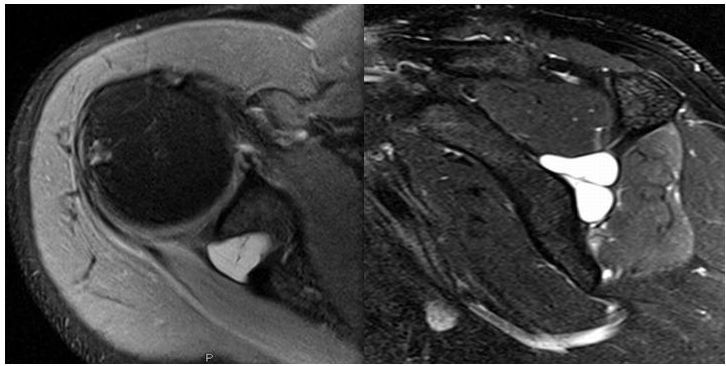
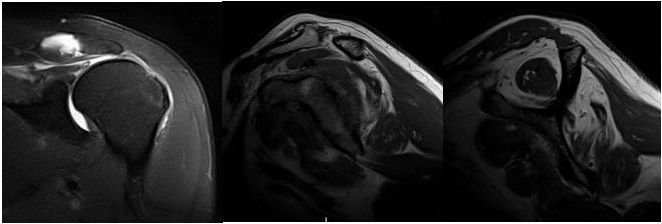
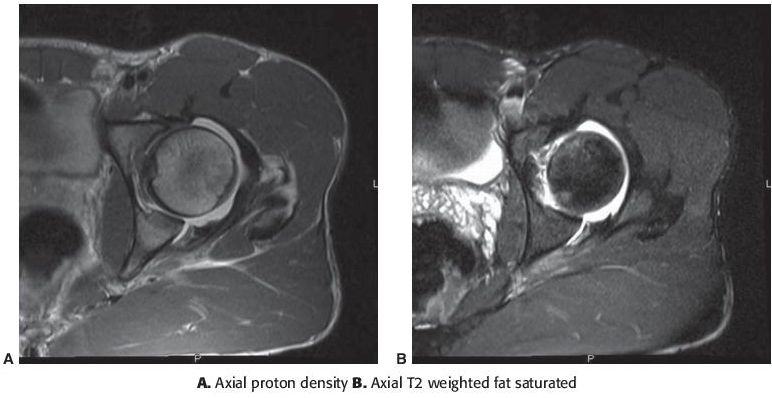
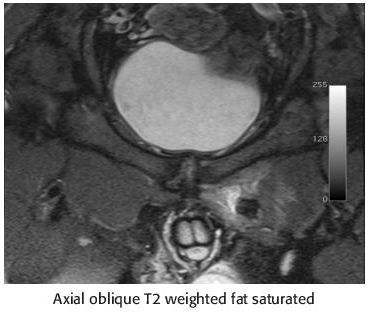
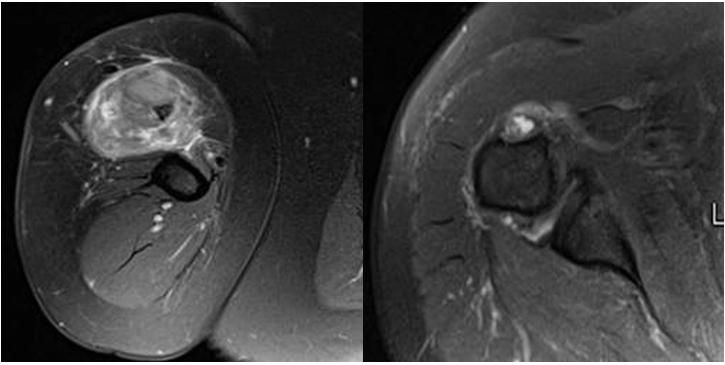
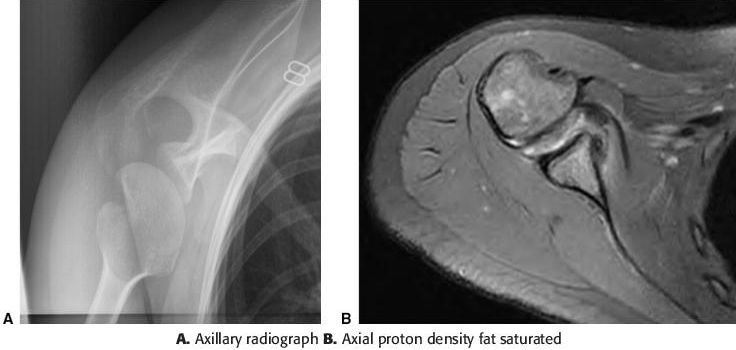
4a Axial and oblique sagittal MR images of the shoulder are provided. The imaged paralabral cyst is located within what anatomic space?
A. Quadrilateral space
B. Suprascapular notch
C. Rotator interval
D. Spinoglenoid notch
4b Compression of the suprascapular nerve in the spinoglenoid notch classically results in denervation of what muscle or muscles?
A. Supraspinatus
B. Supraspinatus and infraspinatus
C. Infraspinatus
D. Teres minor
E. Teres minor and deltoid
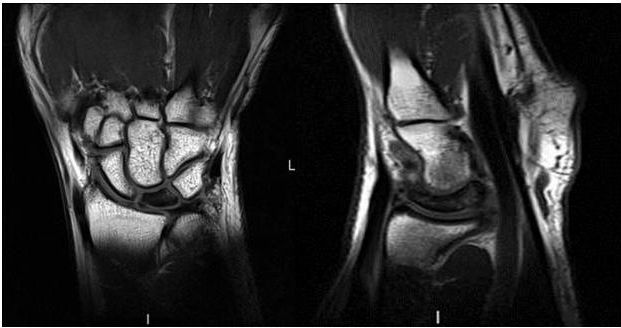
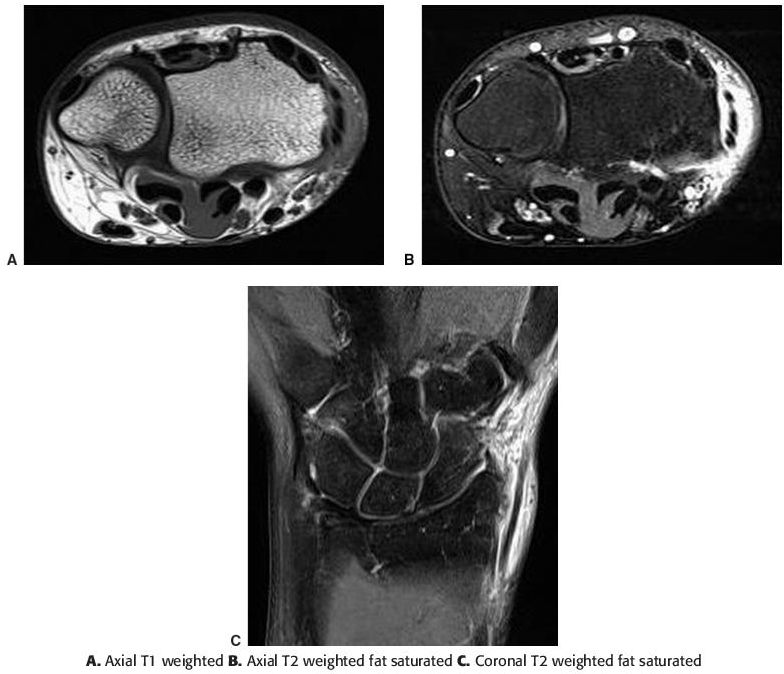
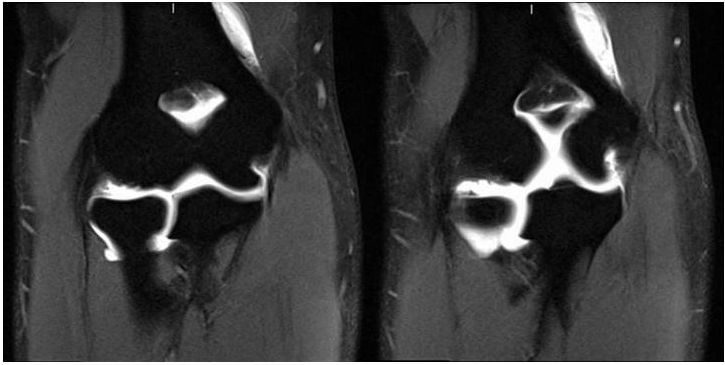
5 Coronal and sagittal T1-weighted images of the wrist are provided. What wrist abnormality is frequented associated with the imaged pathology?
A. Ulnar positive variance
B. Lunotriquetral coalition
C. Ulnar negative variance
D. Distal radioulnar impingement
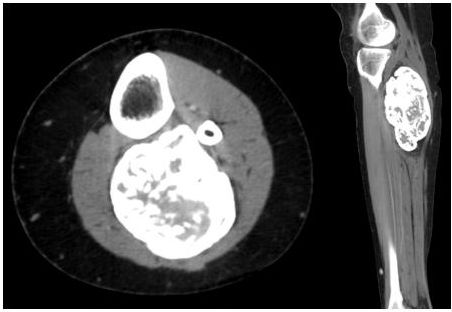
6 A 32-year-old male presented 18 months after surgery with the following CT scan. What is the most likely diagnosis?
A. Heterotopic ossification
B. Parosteal osteosarcoma
C. Tumoral calcinosis
D. Osteochondroma
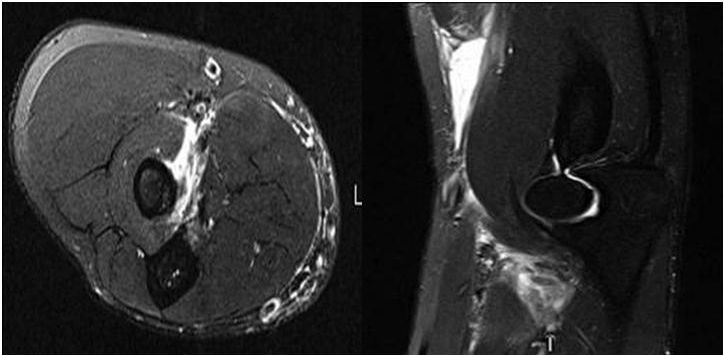
7a Axial and sagittal T2-weighted fat-suppressed images of the elbow are provided. The images depict what abnormality?
A. Bicipitoradial bursitis
B. Brachialis tendon tear
C. Biceps tendon tear
D. Cephalic vein thrombus
7b What structure can prevent proximal retraction of the biceps tendon, even if complete disruption of the tendon has occurred?
A. Biceps tendon sheath
B. Brachialis tendon
C. Lacertus fibrosis
D. Bicipitoradial bursa
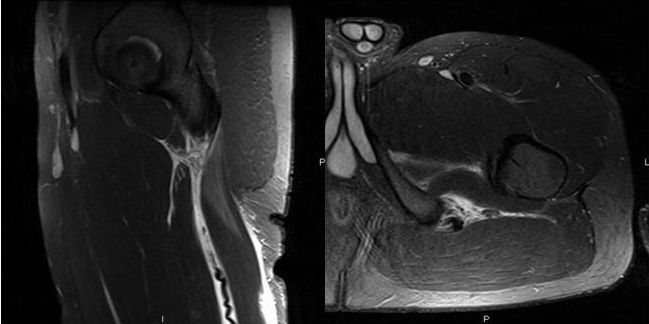
8 The provided image demonstrates avulsion of what tendinous insertion?

A. Rectus femoris
B. Gluteus medius
C. Iliopsoas
D. Rectus abdominis
E. Sartorius
9 Radiographs of the right forearm demonstrate a combination of injuries that are commonly referred to as

A. Monteggia fracture.
B. Galeazzi fracture.
C. Essex-Lopresti fracture.
D. Barton fracture.
E. Smith fracture.
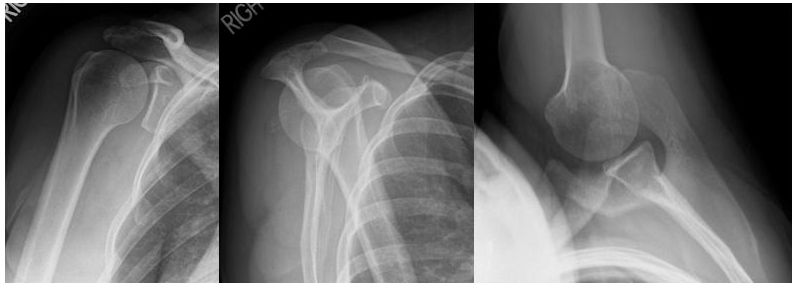
10 What is the most common cause of posterior shoulder dislocation in adult patients?
A. Fall on outstretched hand
B. Direct posterior blow
C. Iatrogenic
D. Seizure
11 A lateral radiograph of the right foot is provided. These findings are concerning for injury to the ligament that spans what space?

A. Lateral cuneiform and fifth metatarsal base
B. Intermediate cuneiform and first metatarsal base
C. Medial cuneiform and second metatarsal base
D. Medial and intermediate cuneiforms
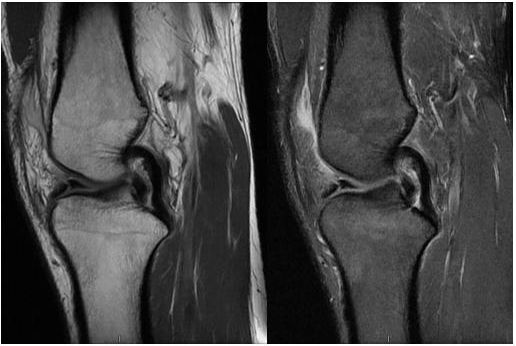
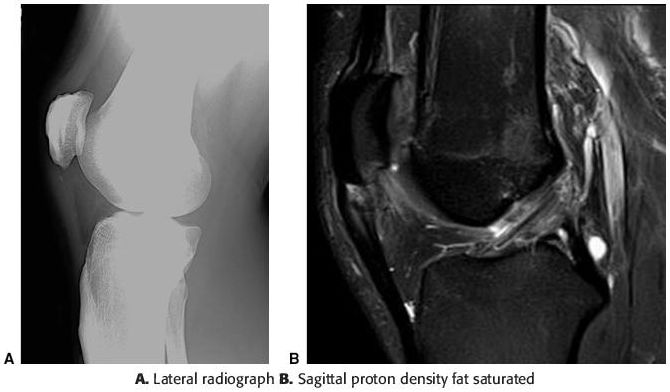
12 A cross-table lateral view of the left knee is provided. Further imaging should be performed primarily to exclude which of the following abnormalities?

A. Anterior cruciate ligament injury
B. Occult fracture
C. Lateral patellar dislocation
D. Medial meniscus tear
13 A patient presents to the emergency department with acute foot pain following a sports injury. Based on the radiograph below, what is the best diagnosis?

A. Jones fracture
B. Fifth metatarsal base avulsion fracture
C. Proximal diaphyseal stress fracture
D. Salter-Harris type 1 fracture
E. Salter-Harris type 2 fracture
14 The imaged pathology affects which of the following extensor tendons?
A. Extensor carpi radialis brevis
B. Extensor pollicis longus
C. Extensor carpi ulnaris
D. Extensor digitorum
E. Extensor pollicis brevis
15 Anterior “kissing contusions” in the knee are seen with which of the following injury mechanisms?
A. Pivot shift
B. Dashboard
C. Hyperextension
D. Clipping
E. Lateral patellar dislocation
16 The following patient presented with shoulder pain. Based on the imaging findings, the patient most likely participates in which of the following activities?

A. Baseball pitching
B. Weight lifting
C. American football
D. Gymnastics
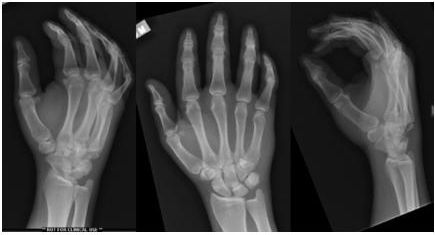
17 A 20-year-old male presents to the emergency department complaining of hand pain and swelling after a fall. Which of the following statements is true regarding his condition?
A. There is a high association with metacarpophalangeal dislocation.
B. Carpometacarpal dislocation without fracture is rare.
C. Carpometacarpal dislocation most commonly occurs volarly.
D. One view is usually sufficient to make the diagnosis.
18 Which pattern of dislocation most commonly occurs at the glenohumeral joint?
A. Anterior infracoracoid
B. Anterior subglenoid
C. Intrathoracic
D. Posterior
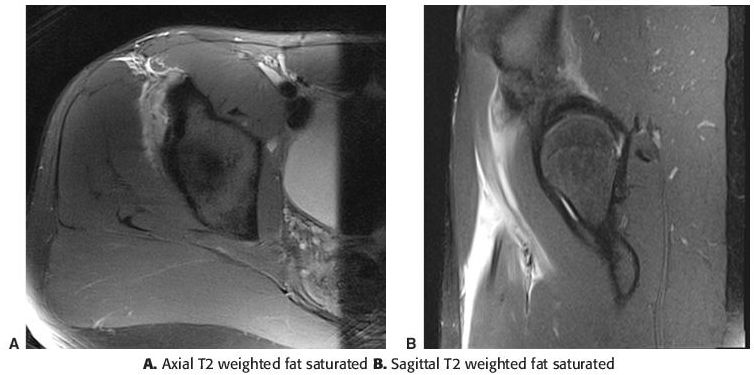
19 An 18-year-old male has an MRI performed after an acute kicking injury and right hip pain. What is the diagnosis?
A. Stress fracture
B. Acetabular labral tear
C. Sartorius tendon tear
D. Rectus femoris tendon tear
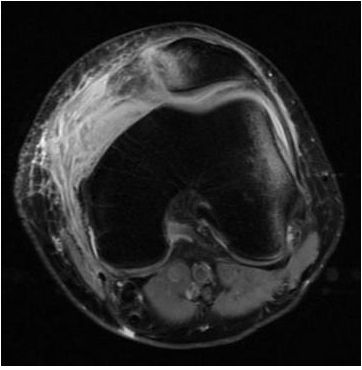
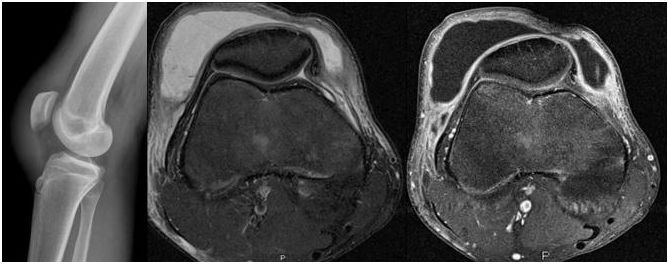
20 A 14-year-old female presents to her pediatrician with acute knee pain following a soccer injury. An axial T2-weighted MR image is provided below. Which of the following would predispose a patient to this type of injury?
A. Iliotibial band friction syndrome
B. Trochlear dysplasia
C. Patella baja
D. Vastus medialis muscle hypertrophy
E. Osgood-Schlatter disease
21 A lateral radiograph of the cervical spine is provided. Which of the following is true regarding the imaged pathology?

A. Results from abrupt hyperextension.
B. More commonly involves the upper cervical spine.
C. Categorized with the Anderson-D’Alonzo classification system.
D. The injury is mechanically stable.
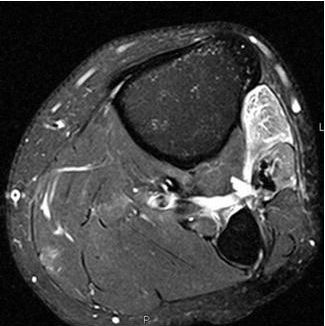
22 A 44-year-old presents with acute onset of pain and swelling of the calf. Axial and coronal T1- and T2-weighted MR images are provided. What is the most likely diagnosis?
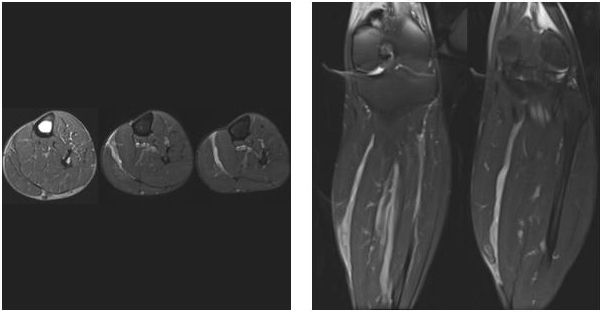
A. Rupture of the medial head of gastrocnemius muscle
B. Rupture of the soleus muscle
C. Dissecting popliteal cyst
D. Rupture of the plantaris tendon
E. Venous varicosity
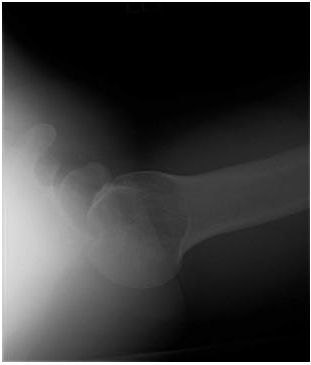
23 A 30-year-old male presents to the emergency department with shoulder pain. Based on the radiograph below, what is the diagnosis?

A. Anterior shoulder dislocation
B. Luxatio erecta
C. Hill-Sachs lesion
D. Posterior shoulder dislocation
E. Reverse Hill-Sachs lesion
24a In addition to tendinopathy, diabetes, steroid use, and connective tissue disorders, what factor might predispose a patient to suffer the injury pictured in the following MRI?
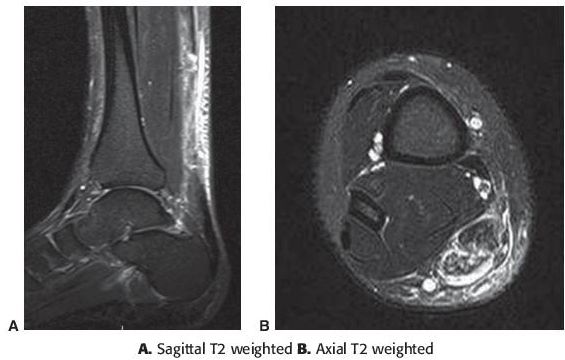
A. Heavy ethanol use
B. Human immunodeficiency virus
C. Recent fluoroquinolone use
D. Hepatitis C
E. Recent penicillin use
24b Achilles tendon tears are most likely to occur at which location?
A. Calcaneal insertion
B. Myotendinous junction
C. Midsubstance
D. Intrasubstance
25 The unopposed action of which tendon causes proximal retraction of the larger fracture fragment in the injury pictured below?

A. Abductor pollicis
B. Flexor pollicis longus
C. Flexor digitorum profundus
D. Extensor pollicis longus
26 The acetabular labrum is most commonly torn in which quadrant?
A. Anterior superior
B. Posterior superior
C. Anterior inferior
D. Posterior inferior
27 Which of the following acetabular fractures involves the iliac wing?
A. Transverse
B. Posterior wall
C. T shaped
D. Both column
E. Transverse with the posterior wall
28 A 17-year-old male football player is referred to radiology for MR arthrogram of the shoulder. The patient reports a remote anterior subluxation event, and the clinician is concerned that the patient may have an anterior inferior labral tear. Which of the following positions will improve visualization of the anterior inferior labrum?
A. Flexion, adduction, and internal rotation
B. Flexion, abduction, and supination
C. Abduction and external rotation
D. Arm neutral with internal rotation
29 What is the most common morphology of the meniscal tear depicted below?
A. Vertical longitudinal
B. Horizontal cleavage
C. Horizontal oblique
D. Radial
30 Complete disruption of which ligament classifies the imaged pathology as a grade III injury as opposed to a grade II injury?

A. Acromioclavicular ligament
B. Coracoclavicular ligament
C. Coracoacromial ligament
D. Coracohumeral ligament
31 Which of the following knee structures should be closely evaluated for an injury, given the imaging finding below?

A. Patellar tendon
B. Posterolateral corner
C. Lateral meniscus
D. Proximal tibiofibular joint
E. Popliteal artery
32 Additional views of the left shoulder may reveal which finding in the following patient?
A. Humeral head locked in external rotation on AP images
B. Increased distance between the articular cortex of the humeral head and glenoid rim
C. Impaction fracture of the posterolateral humeral head
D. Fracture of the anteroinferior glenoid
33 In the injury pictured, entrapment of the ulnar collateral ligament superficial to what structure may result in a Stener lesion, resulting in the need for surgical management?

A. Adductor aponeurosis
B. Radial collateral ligament
C. Extensor hood
D. Flexor pollicis longus
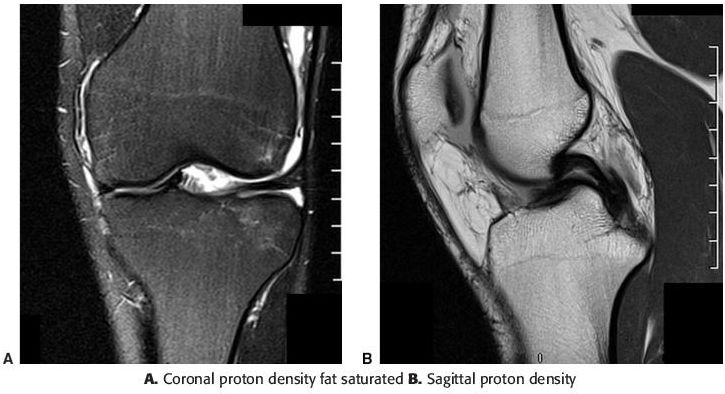
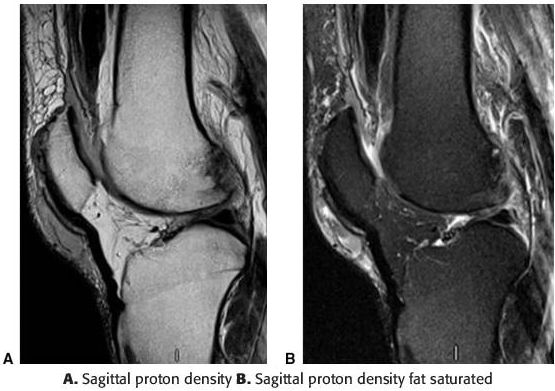
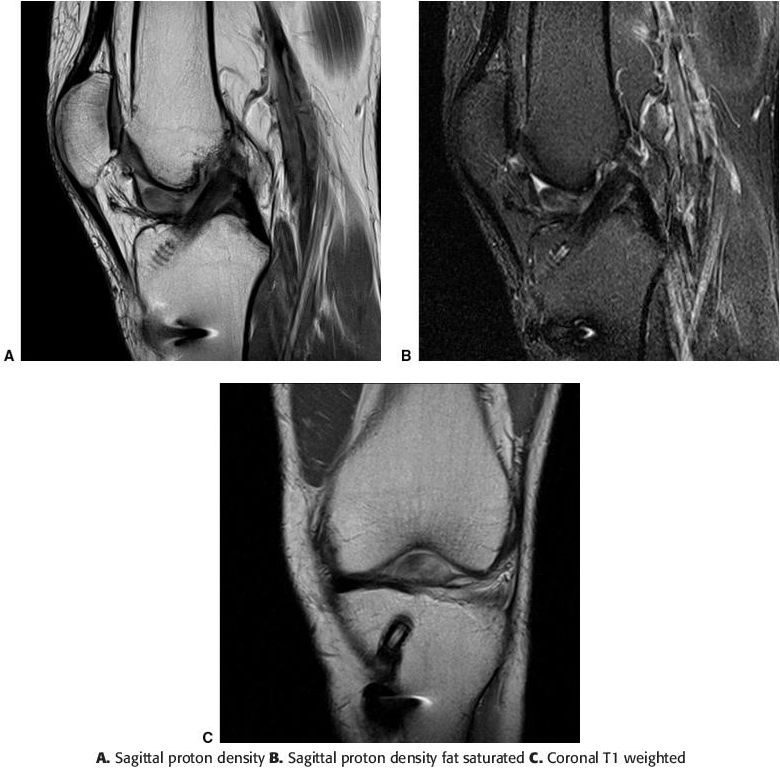
34 A patient complains of persistent knee pain following repeated hyperextension injuries experienced while playing basketball 2 months prior. Sagittal proton density and proton density fat-saturated images through the intercondylar notch are provided. Imaging findings are classic for which of the following injuries?
A. Bucket handle tear of the lateral meniscus
B. Radial tear of the medial meniscus
C. Bucket handle tear of the medial meniscus
D. Partial-thickness tear of the posterior cruciate ligament
35 A19-year-old female runner presents with acutely worsening hip pain. What grade stress injury/stress fracture is depicted in the coronal T2-weighted fat-saturated MR image below?

A. Grade 0
B. Grade 1
C. Grade 2
D. Grade 3
E. Grade 4
36 If emergent surgical management of the imaged injury is not performed, what additional radiologic study should be performed next?

A. MRI of the knee without contrast
B. MRI of the knee with contrast
C. CT angiography of the lower extremity
D. Noncontrast CT of the lower extremity
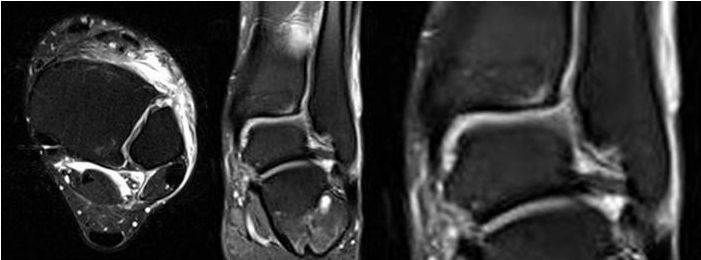
37a A frontal ankle radiograph is provided. Which modality is best suited to estimate the stability of this lesion?

A. CT
B. Ultrasound
C. Tc-99m bone scan
D. MRI
37b MRI findings that would indicate that the above osteochondral lesion is unstable would include
A. fluid signal interface with the donor bone.
B. granulation tissue interface with the donor bone.
C. absence of adjacent cyst-like change.
D. overlying cartilage fissure.
38 What is the prevailing mechanism responsible for the injury pictured below?

A. Hyperextension of the proximal interphalangeal joint
B. Hyperflexion of the proximal interphalangeal joint
C. Avulsion of the flexor digitorum profundus tendon
D. Avulsion of the central slip of the extensor digitorum tendon
39 After a fall on an outstretched hand, a patient complains of elbow pain. Radiographs were obtained in the emergency department. Based on the radiographs, what imaging study should be performed next in the emergent setting?

A. MRI
B. CT
C. Stress radiographs
D. Ultrasound
40 An axial proton density fat-saturated MR image of the upper leg is provided. Injury to what structure could result in the findings below?
A. Tibial nerve
B. Peroneal nerve
C. Popliteal nerve
D. Sciatic nerve
41 Which of the following is the first radiographic manifestation of fracture healing?
A. Callus formation about the fracture site
B. Filling in of callus between the fracture fragments
C. Widening of the fracture line with blurring of fracture margins
D. Demineralization of the adjacent bone around the fracture
42 An oblique radiograph of the left foot is provided. Avulsion of what structure could produce these findings?

A. Peroneus longus
B. Abductor digiti minimi
C. Lateral plantar aponeurosis
D. Peroneal retinaculum
43a Coronal T2-weighted fat-saturated and sagittal T1-weighted MR images of the shoulder are provided. Which of the following best describes the imaging findings?
A. Full-thickness rotator cuff tear with fatty atrophy of the infraspinatus
B. Full-thickness rotator cuff tear with fatty atrophy of the teres minor
C. Full-thickness rotator cuff tear with fatty atrophy of the subscapularis
D. Full-thickness rotator cuff tear with fatty atrophy of the deltoid
43b Rotator cuff tears most commonly involve which tendon?
A. Supraspinatus
B. Subscapularis
C. Infraspinatus
D. Teres minor
44 The 3D CT images below demonstrate the most common mechanism for ankle fracture. What is the mechanism, according to the Lauge-Hansen classification system?

A. Supination adduction
B. Supination external rotation
C. Pronation external rotation
D. Pronation abduction
45 A single axial CT image of the cervical spine is provided. The imaging findings are consistent with what unstable cervical spine injury?

A. Flexion teardrop fracture
B. Bilateral interfacetal dislocation
C. Unilateral perched facet
D. Cervical burst fracture
46 The Pellegrini-Stieda lesion indicates injury to which structure?
A. ACL
B. PCL
C. LCL
D. MCL
47a An 18-year-old hockey player complains of pain after sustaining an injury. Where is the injury?

A. Right hip
B. Left hip
C. Sacrum
D. Pubic symphysis
E. Soft tissues
47b Based on the MR images, what is the most likely mechanism of injury?
A. Anterior dislocation
B. Posterior dislocation
C. Internal rotation
D. External rotation
48 A 47-year-old male suffered high-voltage electrical burn injuries to his feet bilaterally when a metallic tent pole he was assembling contacted a power line. Which of the following is true regarding the imaging findings associated with musculoskeletal thermal trauma?

A. Frostbite-related acroosteolysis most commonly involves the thumb.
B. The physes of skeletally immature patients are relatively resistant to thermal trauma.
C. Resulting muscular fatty atrophy will manifest as areas of T1 prolongation on MRI.
D. Imaging findings may include dystrophic calcification or heterotopic ossification.
49 The combination of injuries seen on the provided radiographs of the right elbow and wrist has been named

A. Essex-Lopresti fracture.
B. Monteggia fracture.
C. Galeazzi fracture.
D. nightstick fracture.
50 A fracture in which region of the scaphoid is most susceptible to developing avascular necrosis?
A. Proximal pole
B. Waist
C. Distal pole
D. Tubercle
51a A frontal radiograph of the knee is provided. This finding has a >90% association with injury to what structure?

A. Biceps femoris tendon
B. Popliteus tendon
C. Anterior cruciate ligament
D. Posterior cruciate ligament
E. Lateral meniscus
51b A mirror image injury to that seen in 51a can also occur, with avulsion of the tibial attachment of the capsular portion of the deep medial collateral ligament. This so-called reverse Segond fracture has a high association with injury to what structure?
A. Semimembranosus tendon
B. Medial head of gastrocnemius
C. Anterior cruciate ligament
D. Posterior cruciate ligament
E. Lateral meniscus
52 Which of the following proximal femoral fractures is most susceptible to avascular necrosis?
A. Intertrochanteric
B. Subtrochanteric
C. Trochanteric
D. Subcapital
53 A 45-year-old man complains of shoulder pain after a fall. Based on the images below, what is the best diagnosis?
A. Sequela of anterior dislocation
B. Sequela of posterior dislocation
C. Nondisplaced fracture
D. Normal variant
54 A 22-year-old college football player experiences acute groin pain after an injury. From the single provided image below, what is the diagnosis?
A. Acute right-sided athletic pubalgia
B. Acute left-sided athletic pubalgia
C. Right-sided inguinal hernia
D. Left-sided inguinal hernia
E. Stress fracture of the pubis
55 Which of the following nerves is most likely entrapped in the clinical setting of forearm pain with weakness of the extensors and preserved sensation?
A. Median nerve
B. Radial nerve
C. Ulnar nerve
D. Anterior interosseous nerve
E. Posterior interosseous nerve
56 A 19-year-old basketball player presents with chronic anterior knee pain. Based on the imaging findings below, which clinical entity is demonstrated?
A. Runner’s knee
B. Jumper’s knee
C. Hoffa syndrome
D. Tennis leg
57 A 19-year-old male presents with a radial side mass and remote history of trauma to the elbow. Radiographs reveal only soft tissue swelling. The ultrasound images below depict what type of foreign body?
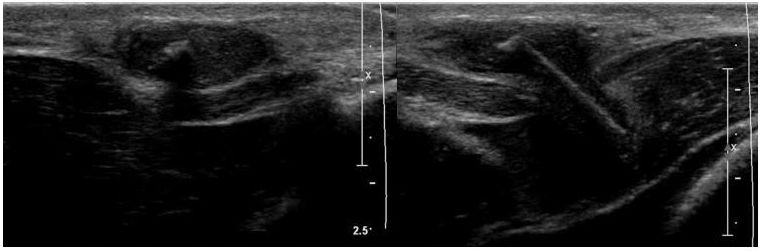
A. Metal
B. Stone
C. Wood
D. Glass
58 The patient suffered an injury resulting in forceful hyperflexion of the distal phalanx of the small finger. Retraction of the avulsed fragment is the result of the action of which tendon?

A. Extensor digiti minimi
B. Flexor digitorum superficialis
C. Flexor digitorum profundus
D. Extensor carpi ulnaris
E. Extensor indicis
59a Axial T2-weighted fat-saturated MR images of the glenohumeral joint and midhumerus are provided. The images depict what abnormality?
A. Long head of biceps tendon rupture
B. Pectoralis major tendon rupture
C. Short head of biceps tendon rupture
D. Coracobrachialis tendon rupture
59b Long head of biceps tendon rupture most commonly occurs in what location?
A. Distal radial attachment
B. Proximal intra-articular portion
C. Proximal intertubercular portion
D. Lacertus fibrosis
60 Based on the findings below, what was the most likely mechanism of injury?
A. Direct anterior impaction
B. Anterior dislocation
C. Posterior dislocation
D. Contrecoup injury
61 A patient presents to the emergency department following an MVC. Which of the following is true regarding the imaged fracture complication?

A. Most commonly occurs following lumbar spine burst fractures.
B. Can be associated with petechial rash, hypoxia, and altered mental status.
C. CT angiography is usually highly specific for the diagnosis of this entity.
D. VQ scan usually shows large central segmental mismatched perfusion defects.
62 A collegiate football player suffered a foot injury while practicing. Radiographs were interpreted as normal, and an MRI was subsequently performed. The requisition states, “concern for Lisfranc injury.” What is the actual diagnosis?

A. Flexor hallucis longus tendon tear
B. Abductor hallucis tendon tear
C. Plantar plate injury
D. Intersesamoid ligament tear
63 A 25-year-old runner complains of lateral knee pain that is worse with activity. Radiographs were performed and were interpreted as normal. Two images from an MR are provided below. What is the correct diagnosis?

A. Iliotibial band tear
B. Iliotibial band syndrome
C. Vastus lateralis muscle tear
D. Bone contusion
E. Fibular collateral ligament tear
64 Sublabral foramen and Buford complex, anatomic variants of the glenoid labrum, occur in which quadrant of the labrum?
A. Posteroinferior
B. Posterosuperior
C. Anteroinferior
D. Anterosuperior
65 A 25-year-old patient complains of wrist pain and swelling after a fall. Three radiographs of the wrist are provided. What is the most likely diagnosis?

A. Perilunate dislocation
B. Lunate dislocation
C. Transscaphoid perilunate dislocation
D. Scaphocapitate fracture dislocation
66 3D CT images of the glenoid are provided. What imaging criterion is commonly used as a cutoff to determine the need for surgical fixation or bone grafting as a means of restoring stability?

A. 10% glenoid surface bone loss
B. 25% glenoid surface bone loss
C. 50% glenoid surface bone loss
D. 75 % glenoid surface bone loss
67 A patient presents with inability to extend the knee following an injury. Which of the following is true regarding the imaged pathology?
A. May be associated with patella alta.
B. Partial-thickness injuries most commonly involve the vastus medialis.
C. Both partial- and full-thickness tears are usually managed conservatively.
D. May be associated with avulsion fractures of the superior patella.
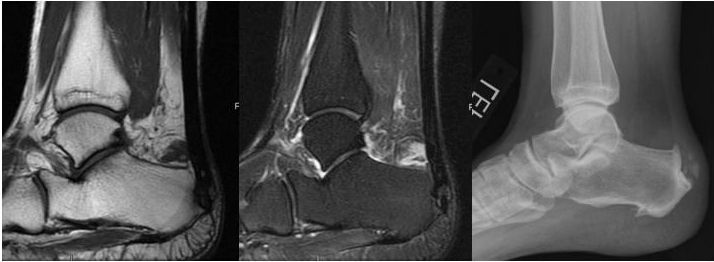
68a T1-weighted and T2-weighted fat-saturated MR images of the ankle are provided, as well as a lateral radiograph. Which term correctly describes osseous excrescences at the calcaneal insertion of the Achilles tendon and the plantar fascia?
A. Osteophyte
B. Periostitis
C. Enthesophyte
D. Osteochondrosis
68b The provided images suggest what diagnosis?
A. Sever disease with retrocalcaneal bursitis
B. Calcaneal stress fracture with retrocalcaneal bursitis
C. Haglund deformity with retrocalcaneal bursitis
D. Plantar fasciitis with retrocalcaneal bursitis
69a A 20-year-old collegiate athlete presented for imaging following an injury suffered during a football game. Sagittal and axial T2-weighted fat-saturated MR images demonstrate injury to the origin of what structure?
A. Gluteus medius tendon
B. Adductor longus tendon
C. Hamstring muscle complex tendons
D. Gluteus maximus tendon
E. Iliopsoas tendon
69b What specific hamstring muscle complex tendon injury is depicted in the images above?
A. Biceps femoris
B. Semimembranosus
C. Semitendinosus
D. Sartorius
70 Which of the following structures represents boundaries or contents of the rotator interval of the shoulder?
A. Short head of the biceps tendon
B. Middle glenohumeral ligament
C. Coracoclavicular ligament
D. Superior glenohumeral ligament
E. Coracoacromial ligament
F. Inferior glenohumeral ligament
71 A 45-year-old female complains of elbow pain. Based on the T2-weighted fat-saturated MR images, which choice below correctly localizes the abnormality?
A. Common extensor origin
B. Common flexor origin
C. Ulnar collateral ligament
D. Radial collateral ligament
72 A 16-year-old high school wrestler presents with a painful anterior knee mass. A lateral knee radiograph is provided, as well as an axial T2-weighted fat-saturated and axial T1-weighted fat-saturated postcontrast MR image. Which of the following correctly identifies the site of the abnormality?
A. Suprapatellar bursa
B. Deep infrapatellar bursa
C. Pes anserine bursa
D. Prepatellar bursa
E. Superficial infrapatellar bursa
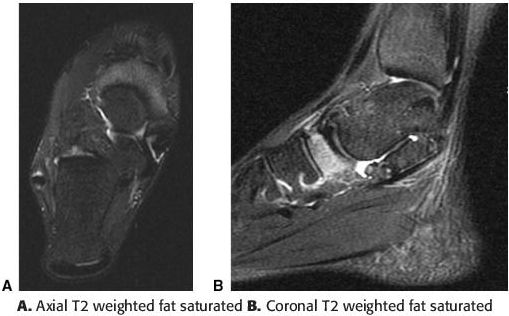
73 Axial and coronal T2-weighted fat-saturated MR images of a football player who sustained an ankle injury are shown below. What is the diagnosis?
A. Anterior talofibular ligament tear
B. Posterior talofibular ligament tear
C. Anteroinferior tibiofibular ligament tear
D. Posteroinferior tibiofibular ligament tear
E. Calcaneofibular ligament tear
74 The imaged pathology most commonly occurs at what specific site in the knee in adolescent patients?

A. Lateral weight-bearing aspect of the medial femoral condyle
B. Medial weight-bearing aspect of the medial femoral condyle
C. Lateral weight-bearing aspect of the lateral femoral condyle
D. Medial weight-bearing aspect of the lateral femoral condyle
75 A 50-year-old complains of persistent pain following a left wrist injury. The initial radiographs of the wrist at the time of injury, 6-week follow-up radiograph, and 6-week follow-up CT scan are presented. What complication of the injury is shown in the 6-week follow-up radiograph and CT scan?

A. Reflex sympathetic dystrophy
B. Fracture nonunion
C. Hardware failure
D. Avascular necrosis
76a PA and lateral radiographs of the wrist are obtained after a patient suffers a fall on an outstretched hand. What is the diagnosis?

A. Perilunate dislocation
B. Scapholunate dissociation
C. Lunate dislocation
D. Midcarpal dislocation
76b Lesser arch injuries of the wrist progress through the following joint spaces in a predictable pattern. Which of the following choices correctly orders the injury progression, from least to greatest severity?
A. Scapholunate; lunotriquetral; lunocapitate
B. Lunotriquetral; lunocapitate; scapholunate
C. Scapholunate; lunocapitate; lunotriquetral
D. Lunocapitate; lunotriquetral; scapholunate
77 A high school sprinter complains of several weeks of ankle pain and is referred for MR imaging. Based on the images below, what is the most appropriate management of this patient?
A. External fixation
B. Prophylactic internal fixation
C. Immobilization and non–weight bearing
D. No treatment necessary, return to sprinting
78 A 61-year-old male was involved in a farming accident. Bedside probing of the wound demonstrates extensive associated soft tissue injury. Initial management of the fracture will likely consist of which of the following?

A. Intramedullary nail
B. External fixation
C. Plate fixation
D. Interfragmentary screws
79 A 22-year-old college student presents with knee pain with extension after anterior cruciate ligament reconstruction. The referring physician is concerned for a tear of the graft. What is the diagnosis?
A. Anterior cruciate graft tear
B. Posterior cruciate ligament tear
C. Meniscus tear
D. Arthrofibrosis
80 Two sequential coronal T1-weighted fat-saturated images from an elbow arthrogram are provided. What is the prevailing mechanism responsible for the injury depicted?
A. Repetitive excessive varus stress
B. Hyperextension injury
C. Distraction injury
D. Repetitive excessive valgus stress
ANSWERS AND EXPLANATIONS
1 Answer A. Pivot shift injury occurs when there is a valgus load applied to the knee while the knee is in various states of flexion. The knee flexion is combined with external rotation of the tibia or internal rotation of the femur. This injury is commonly seen in American football players. The resultant bone contusions are located at the lateral femoral condyle and posterolateral margin of the tibial plateau. The contusions occur after the ACL tears and allow anterior subluxation of the tibia with respect to the femur.
Reference: Sanders TG, Medynski MA, Feller JF, et al. Bone contusion patterns of the knee at MR imaging: footprint of the mechanism of injury. Radiographics. 2000;20:S135–S151.
2 Answer E. The extensor tendons are the dorsal tendons of the wrist and are superficial to the capsule of the wrist. They extend to insert on the carpal bones and phalanges. There are six extensor compartments, which are numbered from the radial to ulnar direction. The compartments are best delineated on axial sequences. Compartment I is composed of the abductor pollicis longus and extensor pollicis brevis tendons and is located along the lateral border of the radius. Compartment II contains the extensor carpi radialis longus and extensor carpi radialis brevis tendons. Compartment II rests along the dorsal and lateral aspect of the radius. Compartment III includes the extensor pollicis longus tendon. Compartment IV is composed of the extensor digitorum and extensor indicis tendons with a shared tendon sheath. The extensor digiti minimi tendon is in Compartment V. Compartment VI contains the extensor carpi ulnaris. Compartments II and III are separated by Lister tubercle, a bony ridge at the dorsal radius.
Reference: Stein JM, Cook TS, Simonson S, et al. Normal and variant anatomy of the wrist and hand on MR imaging. Magn Reson Imaging Clin N Am 2011;19:595–608.
3 Answer B. The provided radiographs demonstrate medial clear space widening and posterior malleolar irregularity. There is no fibular fracture on the provided images. The medial clear space widening indicates deltoid ligament injury. With deltoid ligament injury and a posterior malleolar fracture, the mechanism of injury is pronation–lateral rotation by the Lauge-Hansen classification. A radiograph of the tibia/fibula should be performed with these findings as the posterior malleolar fracture classifies this injury as stage IV. If there is no posterior malleolus fracture, the injury is pronation–lateral rotation stage III. The fibular fracture in pronation–lateral rotation injuries typically occurs anywhere from 6 cm proximal to the tibial plafond to the fibular neck.
Reference: Arimoto HK, Forrester DM. Classification of ankle fractures: an algorithm. AJR Am J Roentgenol. 1980;135:1057–1063.
4a Answer D. Images show a T2-weighted, hyperintense cystic mass within the spinoglenoid notch, without extension into the suprascapular notch. The suprascapular notch is noted superior to the spine of the scapula within the suprascapular fossa and is covered by the superior transverse scapular ligament. From the suprascapular fossa, the nerve continues inferiorly and laterally to the spinoglenoid notch, through which it enters the infraspinous fossa. The spinoglenoid notch may be covered by the spinoglenoid ligament in up to 80% of individuals. The quadrilateral space is bounded inferiorly by the teres major, superiorly by the teres minor, laterally by the humeral neck, and medially by the long head of triceps. The rotator interval is the space bounded by the cranial subscapularis and anterior supraspinatus and contains the superior glenohumeral ligament, coracohumeral ligament, and long head of the biceps tendon.
Reference: Sonin A, Manaster BJ, Andrews CL, et al. Diagnostic Imaging: Musculoskeletal: Trauma. Manitoba, Canada: Amirsys; 2010:2:172–173.
4b Answer C. A paralabral cyst in the spinoglenoid notch can impinge upon the suprascapular nerve and result in denervation of the infraspinatus muscle. When the mass extends into the suprascapular notch, branches to both the supraspinatus and infraspinatus muscles may be compressed. Masses or fibrous bands in the quadrilateral space may compress the axillary nerve, resulting in denervation of the teres minor and deltoid. Masses in the rotator interval do not compress the suprascapular or axillary nerve.
Reference: Sonin A, Manaster BJ, Andrews CL, et al. Diagnostic Imaging: Musculoskeletal: Trauma. Manitoba, Canada: Amirsys; 2010:2:172–173.
5 Answer C. The coronal T1-weighted image shows replacement of the expected fatty marrow signal within the lunate by diffuse T1 hypointensity. The lunate demonstrates an abnormal configuration with flattening. These findings are compatible with lunate osteonecrosis, also called Kienböck disease. After AVN of the proximal pole of the scaphoid, the lunate is the most likely carpal bone to undergo osteonecrosis. The injury results from damage to the tenuous blood supply to the bone, usually from chronic repetitive microtrauma such as that occurs in manual laborers. Ulnar negative variance is often associated with this pathology, due to altered force distribution across the lunate. Ulnar positive variance can be associated with ulnolunate abutment syndrome, resulting in tears of the triangular fibrocartilage and ulnolunate degenerative arthrosis. Distal radioulnar impingement refers to impingement of an abnormally shortened distal ulna against the radius proximal to the sigmoid notch.
Reference: Morrison WB, Sanders TG. Problem Solving in Musculoskeletal Imaging. Philadelphia, PA: Mosby; 2008:464–467.
6 Answer A. Heterotopic ossification is formation of bone and cartilage in soft tissue. It is also referred to as myositis ossificans and is a benign entity. Initially, it manifests as a soft tissue mass. Approximately 4 weeks after the insult, osteoid begins to form and there may be periosteal reaction. The bone continues to mature, and after 6 months, cortical bone is present peripherally. There may be internal trabecula. Patients often present with pain, tenderness, swelling, and a palpable mass. Predisposing factors include trauma, surgery, burns, and neurologic insults including spinal cord injury. Patients with a history of hip arthroplasty are at risk for local heterotopic ossification. Of the other answer choices, tumoral calcinosis is also separate from the bone, but the mass is calcified and not ossified. Parosteal osteosarcoma is a low-grade sarcoma that occurs on the surface of bones. An osteochondroma contains mature bone similar to heterotopic ossification, but there is corticomedullary continuity between the normal bone and the osteochondroma. Osteochondromas usually arise from the metaphysis.
Reference: Manaster BJ, Roberts CC, Petersilge CA, et al. Diagnostic Imaging: Musculoskeletal: Non-Traumatic Disease. Manitoba, Canada: Amirsys; 2010:3:262–267.
7a Answer C. Images show edema along the expected course of the distal biceps tendon, with absence of the tendon at its distal attachment onto the radial tuberosity. While the axial images alone could potentially be confused with a tear of the brachialis tendon (so-called climber elbow), the sagittal images clearly demonstrate an intact brachialis muscle and tendon. Bicipitoradial bursitis may be seen in association with biceps tendon tears; however, in bursitis alone, the tendon would remain intact. Cephalic vein thrombosis would present as the absence of a flow void in the expected location of the cephalic vein.
References: Morrison WB, Sanders TG. Problem Solving in Musculoskeletal Imaging. Philadelphia, PA: Mosby; 2008:412.
Sonin A, Manaster BJ, Andrews CL, et al. Diagnostic Imaging: Musculoskeletal: Trauma. Manitoba, Canada: Amirsys; 2010:3:74–79.
7b Answer C. Distal biceps tendon rupture is usually evident clinically. The role of MR imaging is to differentiate partial from complete disruption and to determine the extent of retraction. An intact lacertus fibrosus (bicipital aponeurosis) may prevent proximal retraction of the biceps tendon even if a complete tear has occurred.
References: Morrison WB, Sanders TG. Problem Solving in Musculoskeletal Imaging. Philadelphia, PA: Mosby; 2008:412.
Sonin A, Manaster BJ, Andrews CL, et al. Diagnostic Imaging: Musculoskeletal: Trauma. Manitoba, Canada: Amirsys; 2010:3:74–79.
8 Answer E. The image depicts avulsion of the anterior superior iliac spine, the attachment site of the sartorius. This injury can commonly be seen in kicking athletes and can be the result of a single episode of forceful contraction or repetitive overuse. Other pelvic and hip avulsion injuries include anterior inferior iliac spine (rectus femoris), ischial tuberosity (semimembranosus and semitendinosus), greater trochanter (gluteus medius), and lesser trochanter (iliopsoas). Tear or detachment of the rectus abdominis aponeurosis from the anteroinferior pubic symphysis is one of the several causes of athletic pubalgia, formerly referred to as a sports hernia. A classic teaching is that, in the adult patient, avulsion of the iliopsoas from the lesser trochanter should raise concern for a pathologic fracture.
Reference: Sanders TG, Zlatkin MB. Avulsion injuries of the pelvis. Semin Musculoskelet Radiol. 2008;12:42–53.
9 Answer B. Galeazzi fracture consists of a radial shaft fracture (usually mid- to distal shaft) with an associated distal radioulnar joint dislocation. The Essex-Lopresti fracture is a radial head fracture with dislocation of the distal radioulnar joint. The radial head fracture is usually comminuted. Monteggia fracture/dislocation is an anterior dislocation of the radial head with a fracture of the proximal third of the ulna. Barton fracture is an intra-articular fracture of the distal radius with subluxation or dislocation of the wrist. The fracture may be volar or dorsal. The Smith fracture is also known as the reverse Colles fracture where there is a distal radius fracture without intra-articular extension. There is volar displacement of the distal fracture fragment in the Smith fracture.
References: Hunter TB, Peltier LF, Lund PJ. Radiologic history exhibit. Musculoskeletal eponyms: who are those guys? Radiographics. 2000;20:819–836.
Lee P, Hunter TB, Taljanovic M. Musculoskeletal colloquialisms: how did we come up with these names? Radiographics. 2004;24:1009–1027.
10 Answer D. Shoulder dislocations are most commonly anterior, referring to the location of the humeral head relative to the glenoid fossa. Posterior dislocations are rare, accounting for 2% of shoulder dislocations. Most posterior dislocations can be classified as subacromial and are fixed with the humeral head trapped posterior to the glenoid. There is commonly an associated humeral head fracture. Posterior dislocation is commonly the result of violent muscle contractions in the setting of seizures. The shoulder can also posteriorly dislocate as a result of electric shock or a direct anterior blow to the shoulder. Posterior dislocation can be subtle radiographically. On frontal radiographs of the shoulder, it may manifest as severe internal rotation of the humeral head resembling a light bulb or the rim sign. In the rim sign, there is increased distance between the glenoid and articular surface of the humeral head. Posterior dislocation can also manifest as the trough line sign on frontal radiographs. When the humeral head posteriorly dislocates, it impacts the posterior glenoid. The impaction at the medial humeral head has a linear configuration and is called the trough line sign. This fracture is sometimes referred to as the reverse Hill-Sachs fracture.
References: Gor DM. The trough line sign. Radiology. 2002;224:485–486.
Pope TL, Harris JH. Harris and Harris’ the Radiology of Emergency Medicine. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2013:319–320, 326–328.
11 Answer C. The Lisfranc ligament spans the medial cuneiform-second metatarsal base. This structure is crucial to stabilization of the midfoot and longitudinal arch. The radiographic findings include widening of the space between the first and second metatarsals, abnormal tarsal–metatarsal alignment, and dorsal migration of the metatarsal bases. Injuries are commonly classified as homolateral or divergent based upon the direction of dislocation of the first metatarsal with respect to that of the metatarsals two through five. In Lisfranc injuries, the ligament may avulse from the second metatarsal or medial cuneiform or may tear within its substance without associated fracture.
References: Morrison WB, Sanders TG. Problem Solving in Musculoskeletal Imaging. Philadelphia, PA: Mosby; 2008:702–705.
Pope TL, Harris JH. Harris and Harris’ the Radiology of Emergency Medicine. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2013:962–965.
12 Answer B. A cross-table lateral view of the knee shows a layered joint effusion, with the more lucent-nondependent layer representing lipid. The presence of both blood and fat within the joint space is highly specific for an intra-articular fracture, with the fat layer representing that which has leaked into the joint from the marrow cavity. Further imaging should be performed to identify the fracture, if not seen radiographically.
Reference: Pope TL, Harris JH. Harris and Harris’ the Radiology of Emergency Medicine. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2013:876–877.
13 Answer A. A Jones fracture is defined as a transverse fracture of the fifth metatarsal at the junction of the proximal metaphysis and diaphysis, without extension distal to the level of the fourth and fifth intermetatarsal articulations. A tuberosity avulsion fracture occurs proximal to a Jones fracture and results from avulsion of the peroneus brevis tendon and plantar aponeurosis. The avulsion fracture is the most common proximal fifth metatarsal fracture. A fifth metatarsal proximal diaphyseal stress fracture occurs distal to a Jones fracture and normally is seen within the proximal 1.5 cm of the fifth metatarsal diaphysis. Fifth metatarsal stress fractures are the least common proximal fifth metatarsal fractures.
Reference: Theodorou DJ, Theodorou SJ, Kakitsubata Y, et al. Fractures of proximal portion of fifth metatarsal bone: anatomic and imaging evidence of a pathogenesis of avulsion of the plantar aponeurosis and the short peroneal muscle tendon. Radiology. 2003;226:857–865.
14 Answer E. MR images of the wrist demonstrate fluid within the tendon sheaths of the first extensor compartment and adjacent soft tissue inflammatory changes, findings compatible with de Quervain tenosynovitis. Tenosynovitis involving the abductor pollicis longus and extensor pollicis brevis tendons in this location produces radial wrist pain and swelling. De Quervain tenosynovitis may result from a variety of activities that produce repetitive microtrauma, such as rowing, golfing, or racquet sports. De Quervain tenosynovitis is also referred to as baby wrist overuse syndrome. First extensor compartment inflammation is commonly seen in mothers of newborns due to repeated extension or flexion of the wrist with abduction of the thumb against resistance. This diagnosis can also be made via wrist ultrasound, which would demonstrate fluid within the tendon sheaths of the first extensor compartment and focal increased vascularity.
Reference: Anderson SE, Steinbach LS, De Monaco D, et al. “Baby wrist”: MRI of an overuse syndrome in mothers. AJR Am J Roentgenol. 2004;182:719–724.
15 Answer C. The anterior “kissing contusion” pattern is seen when the anterior aspect of the tibial plateau contacts the anterior aspect of the femoral condyle. Hyperextension can be direct, with force applied to the anterior tibia, or indirect such as in forceful kicking.
Reference: Sanders TG, Medynski MA, Feller JF, et al. Bone contusion patterns of the knee at MR imaging: footprint of the mechanism of injury. Radiographics. 2000;20:S135–S151.
16 Answer B. The radiographic images demonstrate widening of the acromioclavicular joint. There is distal clavicle resorption as evidenced by the irregularity of the distal clavicle best seen on the axillary view. There are several bone fragments along the undersurface of the distal clavicle that may be related to prior coracoclavicular ligament injury. Unilateral distal clavicular osteolysis is usually posttraumatic. Osteomyelitis and metastatic disease or myeloma can also cause unilateral distal clavicular osteolysis. Bilateral distal clavicular osteolysis is more likely the result of systemic conditions including hyperparathyroidism, rheumatoid arthritis, and scleroderma. Posttraumatic osteolysis of the distal clavicle occurs after repetitive microtrauma or acute acromioclavicular joint trauma. Classically, distal clavicular osteolysis is seen in weight lifters as a result of chronic stress at the acromioclavicular joint. Early radiographic findings of distal clavicular osteolysis include swelling of the acromioclavicular joint, joint space widening, distal clavicle demineralization, and loss of the distal clavicle cortex. Over time, the cortical margin can reconstitute. Distal clavicle subchondral cysts are a chronic finding.
Reference: Morrison WB, Sanders TG. Problem Solving in Musculoskeletal Imaging. Philadelphia, PA: Mosby; 2008:336–339.
17 Answer B. The majority of carpometacarpal (CMC) dislocations involve multiple joints. Dislocation of the CMC joints other than the thumb is rare. When CMC dislocation occurs, there is usually an associated fracture due to the strength of the CMC and intermetacarpal ligaments. The index (second) and long (third) finger CMC articulations are relatively immobile, and therefore ring (fourth) and little (fifth) finger CMC dislocations are more common. CMC dislocations can be subtle on the standard three radiographic views of the hand, and CT can be helpful when CMC dislocation is suspected.
Reference: Pope T, Harris J. Harris and Harris’ the Radiology of Emergency Medicine. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2013:433–436.
18 Answer A. The shoulder is the most commonly dislocated joint in the body. Anterior dislocations are far more common than posterior. In the anterior infracoracoid dislocation subtype, the humeral head rests below the coracoid. This pattern is the most common type of dislocation. Dislocation frequently happens at the glenohumeral joint due to the large humeral head articular surface compared to that of the glenoid and due to the relative weakness of the capsule.
Reference: Pope TL, Harris JH. Harris and Harris’ the Radiology of Emergency Medicine. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2013:319–332.
19 Answer D. The images demonstrate extensive edema at the anterior inferior iliac spine. The sagittal image shows no normal rectus femoris tendon fibers extending from the anterior inferior iliac spine. The rectus femoris muscle is a long fusiform muscle with two heads. The direct head originates from the anterior inferior iliac spine, and the indirect head originates from the superior acetabular ridge. Most rectus femoris injuries occur at the myotendinous junction. However, tears at the origin can occur in kicking injuries.
Reference: Gyftopoulos S, Rosenberg ZS, Schweitzer ME, et al. Normal anatomy and strains of the deep musculotendinous junction of the proximal rectus femoris: MRI features. AJR Am J Roentgenol. 2008;190:W182–W186.
20 Answer B. The axial MR image of the knee demonstrates medial patellar facet and lateral femoral condyle bone contusions, as well as disruption of the medial patellofemoral retinaculum. These findings are consistent with the sequela of lateral patellar dislocation. Several risk factors for patellar instability have been identified, including trochlear dysplasia, patella alta, and lateralization of the tibial tuberosity. The medial retinaculum and medial patellofemoral ligament are the most important ligamentous stabilizers of the patella.
References: Diederichs G, Issever AS, Scheffler S. MR imaging of patellar instability: injury patterns and assessment of risk factors. Radiographics. 2010;30:961–981.
Elias DA, White LM, Fithian DC. Acute lateral patellar dislocation at MR imaging: injury patterns of medial patellar soft-tissue restraints and osteochondral injuries of the inferomedial patella. Radiology. 2002;225:736–743.
21 Answer D. The lateral upright radiograph of the cervical spine shows an avulsion fracture of the C7 spinous process, called a clay shoveler’s fracture. This injury occurs as a result of abrupt flexion of the head. The tensed interspinous ligaments of the posterior neck result in avulsion of the spinous process. The clay shoveler’s fracture can occur at C6, C7, and T1. This fracture is mechanically and neurologically stable. Of note, the Anderson-D’Alonzo classification system describes fractures of the dens.
Reference: Pope TL, Harris JH. Harris and Harris’ the Radiology of Emergency Medicine. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2013:190.
22 Answer D. Tears of the proximal myotendinous junction of the plantaris may result in a curvilinear fluid collection or hematoma located between the medial head of gastrocnemius and soleus muscles, as seen in the provided images. The lack of abnormal signal within the gastrocnemius and soleus muscles argues against injury to these structures. A dissecting popliteal cyst can be traced back to its origin between the tendons of the medial head of gastrocnemius muscle and the semimembranosus muscle at the level of the knee. Patients suffering from plantaris tendon injury may sense a “pop” followed by sudden-onset calf pain. Conservative management is the treatment of choice.
Reference: Stoller DW. Magnetic Resonance Imaging in Orthopaedics and Sports Medicine. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2007:006–009.
23 Answer B. Luxatio erecta, or inferior dislocation of the glenohumeral joint, is a rare entity that accounts for ~0.5% of all shoulder dislocations. Although rare, it has a characteristic imaging and clinical presentation, with the shaft of the humerus externally rotated and directed cephalad. Luxatio erecta has a classic clinical presentation with the patient unable to move the arm at the shoulder. The arm is held above the head with the elbow flexed. This hyperabduction injury may result in rotator cuff tear, injury to the brachial plexus, and injury to the axillary artery or vein. Fractures of the greater tuberosity, acromion process, and inferior glenoid rim may also be associated with this injury.
References: Downey EF Jr, Curtis DJ, Brower AC. Unusual dislocations of the shoulder. AJR Am J Roentgenol. 1983;140:1207–1210.
Kothari K, Bernstein RM, Griffiths HJ, et al. Luxatio erecta. Skeletal Radiol. 1984;11:47–49.
24a Answer C. The sagittal T2-weighted fat-saturated MR image demonstrates a full-thickness tear of the Achilles tendon. This injury commonly occurs in middle-aged “weekend warriors” participating in activities requiring sudden forceful plantar flexion. Several factors may predispose to this injury. Systemic disorders such as rheumatoid arthritis, diabetes, and crystalline arthropathies have a proven association with Achilles tendon tears. Of the medications linked to Achilles tendon rupture, steroids and fluoroquinolone antibiotics have the greatest association.
References: Morrison WB, Sanders TG. Problem Solving in Musculoskeletal Imaging. Philadelphia, PA: Mosby; 2008:662–666.
Sode J, Obel N, Hallas J, et al. Use of fluoroquinolone and risk of Achilles tendon rupture: a population-based cohort study. Eur J Clin Pharmacol. 2007;63:499–503.
24b Answer C. In this case, disruption of the tendon has occurred in the most common location, the relatively avascular zone found 2 to 6 cm proximal to the calcaneal insertion.
References: Morrison WB, Sanders TG. Problem Solving in Musculoskeletal Imaging. Philadelphia, PA: Mosby; 2008:662–666.
Sode J, Obel N, Hallas J, et al. Use of fluoroquinolone and risk of Achilles tendon rupture: a population-based cohort study. Eur J Clin Pharmacol. 2007;63:499–503.
25 Answer A. A Bennett fracture is a noncomminuted intra-articular fracture of the base of the thumb metacarpal. The larger fracture fragment is retracted proximally by the unopposed action of the abductor pollicis longus tendon. This injury may require open reduction and internal fixation. A Rolando fracture is a three-part intra-articular fracture of the first metacarpal base and has a worse prognosis than the two-part Bennett fracture.
References: Morrison WB, Sanders TG. Problem Solving in Musculoskeletal Imaging. Philadelphia, PA: Mosby; 2008:495–496.
Pope TL, Harris JH. Harris and Harris’ the Radiology of Emergency Medicine. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2013:429–431.
26 Answer A. Acetabular labral detachments are more common than tears. Most acetabular labral tears are located anterosuperiorly. The anterior superior portion of the acetabular labrum may be affected by femoroacetabular impingement. Posterior acetabular labral tears are much less common and are usually seen in young and athletic patients.
Reference: Blankenbaker DG, Tuite MJ. Acetabular labrum. Magn Reson Imaging Clin N Am. 2013;21:21–33.
27 Answer D. Several systems exist for classification of acetabular fracture, but the Judet-LeTournel system is the most widely accepted. This classification system uses the column principle of the acetabulum. The anterior column is longer and larger and extends from the superior pubic ramus to the iliac wing. The posterior column extends from the ischiopubic ramus to the ilium. There are 10 types of fractures in the Judet-LeTournel system, but the most common (90%) are the both column, T shaped, transverse, transverse with posterior wall, and isolated posterior wall. Both column and T shaped fractures disrupt the obturator ring, and only the both column fracture involves the iliac wing.
Reference: Durkee NJ, Jacobson J, Jamadar D, et al. Classification of common acetabular fractures: radiographic and CT appearances. AJR Am J Roentgenol. 2006;187:915–925.
28 Answer C. When a patient is placed in abduction and external rotation (ABER), the anterior inferior glenohumeral ligament is under tension. This stress on the capsule and anteroinferior labroligamentous complex can produce separation of a tear that will fill with contrast, and thus will be better visualized than on routine neutral positioning.
Reference: Saleem AM, Lee JK, Novak LM. Usefulness of the abduction and external rotation views in shoulder MR arthrography. AJR Am J Roentgenol. 2008;191:1024–1030.
29 Answer A. The coronal proton density fat-saturated MR image demonstrates displaced meniscal tissue in the medial aspect of the intercondylar notch. The sagittal proton density MR image on the right demonstrates the double PCL sign with displaced meniscal tissue in the intercondylar notch. This patient has a bucket handle tear of the medial meniscus. Longitudinal tears, either vertical or horizontal, are the most common types of meniscal tears. In a bucket handle tear, the inner fragment of the torn meniscus is displaced toward the notch. The handle of the bucket is formed by the displaced meniscal fragment with the bucket formed by the peripheral nondisplaced meniscal component.
Reference: Resnick D, Kang HS, Pretterkieber ML. Internal Derangement of Joints. 2nd ed. Philadelphia, PA: Saunders; 2007:1657–1660.
30 Answer B. Injury to the acromioclavicular joint can be classified in regard to which stabilizing ligamentous structures are damaged. In grade I injuries, there is a sprain of the acromioclavicular ligament that is not evident radiographically. With a grade II injury, there is complete disruption of the acromioclavicular ligament resulting in widening of the joint space, typically regarded as exceeding 4 mm. Variable injury to the coracoclavicular ligament can be present in a grade II injury; however, complete disruption is not present. Both grade I and grade II injuries usually respond well to nonsurgical management and should be differentiated from a grade III injury, in which there is complete disruption of the coracoclavicular ligament. This thick and relatively strong ligamentous complex consists of two components: the trapezoid and the conoid. This injury is often evident clinically; however, this can be seen radiographically as elevation of the clavicle and an increased coracoclavicular distance. Some classification systems include additional grades IV–VI, which are beyond the scope of this discussion.
References: Morrison WB, Sanders TG. Problem Solving in Musculoskeletal Imaging. Philadelphia, PA: Mosby; 2008:338–339.
Pope TL, Harris JH. Harris and Harris’ the Radiology of Emergency Medicine. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2013:313–319.
31 Answer B. The frontal radiograph of the knee demonstrates a proximally retracted avulsion fracture of the fibular head, referred to as the arcuate sign. This injury has a high association with injury to the posterolateral corner of the knee. The posterolateral corner structures include the lateral collateral ligament, the fabellofibular ligament, the popliteofibular ligament, the arcuate ligament, the popliteal tendon, and the biceps femoris tendon. If left unrecognized, an injury to the posterolateral corner structures can result in chronic instability. This instability ultimately may lead to failure of anterior cruciate ligament reconstruction.
References: Huang GS, Yu JS, Munshi M et al. Avulsion fracture of the head of the fibula (the “arcuate” sign): MR imaging findings predictive of injuries to the posterolateral ligaments and posterior cruciate ligament. AJR Am J Roentgenol. 2003;180:381–387.
Strub WM. The arcuate sign. Radiology. 2007;244:620–621.
32 Answer B. The axillary view demonstrates posterior dislocation of the humeral head. Additional radiographic findings associated with posterior shoulder dislocation include impaction fracture of the anterior humeral head, opposite of the Hill-Sachs lesion associated with anterior shoulder dislocation in which impaction occurs posterolaterally. With posterior dislocation, the shoulder may be locked in extreme internal rotation on AP images. There may be increased distance between the articular cortex of the humeral head and glenoid known as the positive rim sign; however, the opposite can also occur in which this distance is decreased. A fracture of the posterior glenoid may also be seen, referred to as a reverse Bankart lesion.
Reference: Pope TL, Harris JH. Harris and Harris’ the Radiology of Emergency Medicine. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2013:326–332.
33 Answer A. Gamekeeper thumb refers to an injury of the ulnar collateral ligament (UCL) at the thumb metacarpophalangeal joint (MCP). Currently, the injury is most frequently seen in skiing-related trauma. Mechanistically, the injury results from excessive valgus stress applied across the MCP joint of the thumb. The injury may be associated with avulsion fractures of the distal attachment of the ulnar collateral ligament, as pictured. MRI is often performed with suspected UCL injuries, both to evaluate the degree of injury to the UCL and to determine the presence or absence of a Stener lesion, which requires surgical management. A Stener lesion refers to cases in which the torn and retracted proximal UCL becomes entrapped superficial to the adductor aponeurosis, preventing apposition of the proximal and distal fragments and thus resulting in inadequate healing.
References: Morrison WB, Sanders TG. Problem Solving in Musculoskeletal Imaging. Philadelphia, PA: Mosby; 2008:491.
Pope TL, Harris JH. Harris and Harris’ the Radiology of Emergency Medicine. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2013:431–423.
34 Answer C. Sagittal proton density and proton density fat-saturated images of the knee demonstrate an abnormal band of hypointense tissue within the posterior intercondylar notch anterior to and paralleling the posterior cruciate ligament, the so-called double PCL sign. This finding is seen in the setting of a bucket handle tear of the medial meniscus with meniscal tissue displaced into the posterior intercondylar notch. When a bucket handle tear occurs laterally, which is less common, the double PCL sign does not typically occur because the ACL blocks the fragment from entering the posterior notch. This case also demonstrates a classic example of the double delta or double anterior horn, which represents a bucket handle tear with meniscal tissue flipped anteriorly into the intercondylar notch.
Reference: Morrison WB, Sanders TG. Problem Solving in Musculoskeletal Imaging. Philadelphia, PA: Mosby; 2008:601–604.
35 Answer E. Stress injuries/fractures of bone can be classified on MRI by a five-point system as follows:
Grade 0: Normal study
Grade 1: Subtle periosteal edema
Grade 2: Periosteal edema in addition to marrow edema on T2-weighted fat-saturated images
Grade 3: More extensive periosteal edema; marrow changes on both T2-weighted fat-saturated and T1-weighted sequences
Grade 4: True stress fractures with a fracture line visible on MRI or radiographs
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


