Discontinuity of hemidiaphragm with focal defect (segmental diaphragmatic defect)
Dangling diaphragm sign: Free edge of torn diaphragm curls inward on axial images rather than continuing its normal course parallel to chest wall
Absent diaphragm sign: Absence of diaphragm in expected location without visualization of discrete tear
Herniation of abdominal contents through a discrete diaphragmatic defect
Collar sign: Waist-like narrowing of herniated structure as it extends through diaphragmatic tear
Fallen or dependent viscus sign: Herniated viscus abuts posterior ribs and thoracic wall without intervening lung
Secondary signs of injury include simultaneous presence of pneumothorax and pneumoperitoneum or hemothorax and hemoperitoneum, active extravasation of contrast in or near diaphragm, or injuries to organs lying near diaphragm
PATHOLOGY
• 75% of cases caused by blunt trauma, and 25% caused by penetrating trauma
• Strong association with polytrauma and other major traumatic injuries
CLINICAL ISSUES
• 1-5% of all patients with substantial blunt abdominal or thoracic trauma
• True incidence is likely underestimated, as these injuries may be frequently missed on imaging
• Surgical repair of diaphragm indicated for all diaphragmatic injuries, even when small
(Left) Chest x-ray in a young man following a motor vehicle crash shows a pneumothorax, chest tube, and an NG tube that is curved up toward the chest.
(Right) Axial CT in the same patient shows the typical signs of diaphragmatic injury, including the fallen viscus sign. The stomach lies in the chest. Note that it has “fallen” medially and posteriorly to lie against the posteromedial chest wall. The stomach appears pinched as it traverses the defect in the diaphragm (collar sign).
(Left) Axial CECT shows the stomach in the thorax, and it has “fallen” through the diaphragmatic defect to lie against the posteromedial chest wall. The anterior wall of the stomach directly abuts the lung, and is not confined by the diaphragm.
(Right) Coronal CECT in the same patient demonstrates the stomach extending upward through a diaphragmatic defect.
TERMINOLOGY
Synonyms
• Traumatic diaphragmatic hernia
Definitions
• Diaphragmatic rupture ± herniation of abdominal contents into thorax
IMAGING
General Features
• Best diagnostic clue
Discontinuity of hemidiaphragm with fallen or dependent viscus sign
• Location
90-98% occur on left side (usually posterolateral part of diaphragm, medial to spleen)
– Left hemidiaphragm has weaker pleuroperitoneal membrane, while right hemidiaphragm is protected by liver
• Size
Blunt trauma
– Most tears are large (> 10 cm in length)
Penetrating trauma
– Gunshot wounds (blast injuries) → large defects in diaphragm
Collar sign: Waist-like narrowing of herniated structure as it extends through diaphragmatic tear
– Often easier to appreciate on coronal multiplanar reformats
– May be associated with hump sign: Unusual contour of liver as it extends through diaphragmatic defect, often with a band-like region of hypoperfusion of liver at base of hernia
Fallen or dependent viscus sign: Herniated viscus abuts posterior ribs and thoracic wall without intervening lung
Abdominal contents lateral to diaphragm on axial images
Active extravasation of contrast in or near diaphragm
Secondary signs of injury include simultaneous presence of pneumothorax and pneumoperitoneum or hemothorax and hemoperitoneum, active extravasation of contrast in or near diaphragm, or injuries to organs lying near diaphragm
– Trajectory of penetrating injury can often be surmised from other injuries and ectopic gas, and can increase suspicion for diaphragmatic injury
• Diaphragmatic rupture remains difficult diagnosis on CT, with reported sensitivities as low as 73% and specificities as low as 50%
Multiplanar reformations are critical to diagnosis, and partially explain superior performance of modern MDCT compared to pre-MDCT technology
MR Findings
• Normal diaphragm on T1- and T2WI appears as a continuous hypointense band
Diaphragm is generally easier to visualize on MR than on CT, but MR is usually more appropriate for evaluation of stable patient, not in acute trauma setting
• Imaging findings parallel those on CT
Radiographic Findings
• Radiography
Radiographs are significantly less sensitive than CT for diaphragmatic injury, but may often be initial study performed
– Nonvisualized or abnormal diaphragmatic contour with abnormally elevated hemidiaphragm contour
Upper diaphragmatic contour may be elevated > 6 cm above contralateral hemidiaphragm
Only gold members can continue reading. Log In or Register to continue
 Dangling diaphragm sign: Free edge of torn diaphragm curls inward on axial images rather than continuing its normal course parallel to chest wall
Dangling diaphragm sign: Free edge of torn diaphragm curls inward on axial images rather than continuing its normal course parallel to chest wall Absent diaphragm sign: Absence of diaphragm in expected location without visualization of discrete tear
Absent diaphragm sign: Absence of diaphragm in expected location without visualization of discrete tear

 Fallen or dependent viscus sign: Herniated viscus abuts posterior ribs and thoracic wall without intervening lung
Fallen or dependent viscus sign: Herniated viscus abuts posterior ribs and thoracic wall without intervening lung Secondary signs of injury include simultaneous presence of pneumothorax and pneumoperitoneum or hemothorax and hemoperitoneum, active extravasation of contrast in or near diaphragm, or injuries to organs lying near diaphragm
Secondary signs of injury include simultaneous presence of pneumothorax and pneumoperitoneum or hemothorax and hemoperitoneum, active extravasation of contrast in or near diaphragm, or injuries to organs lying near diaphragm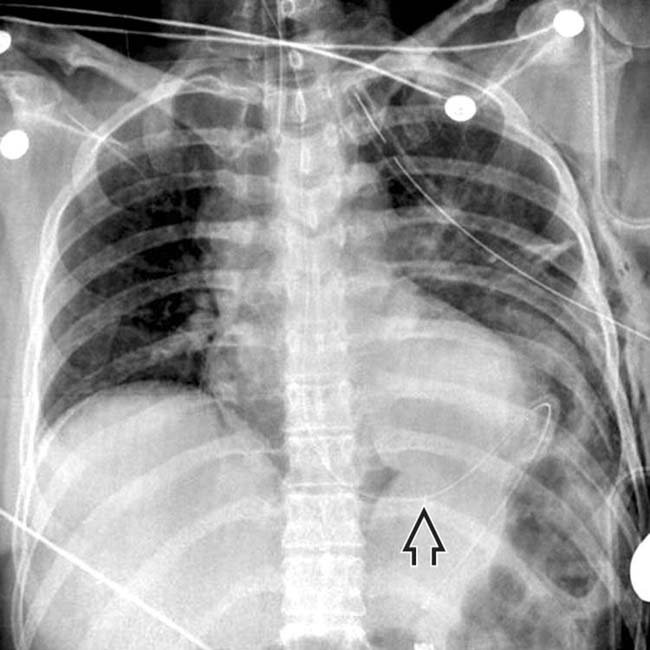
 that is curved up toward the chest.
that is curved up toward the chest.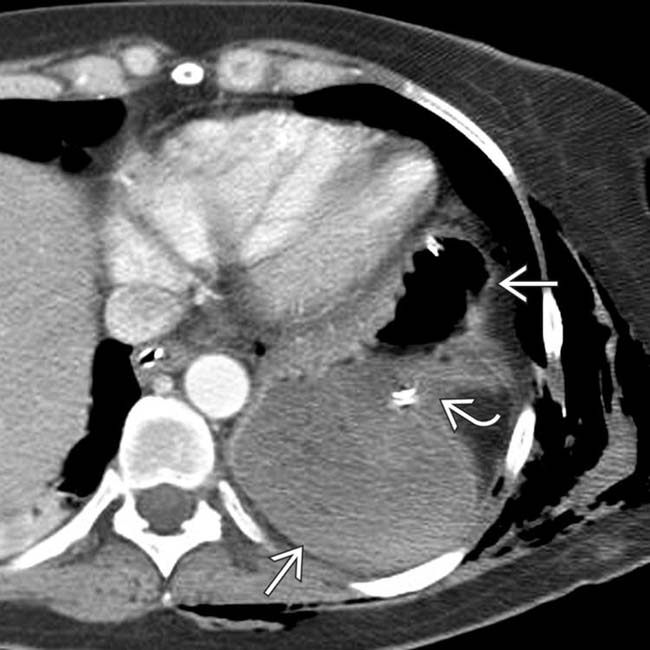
 lies in the chest. Note that it has “fallen” medially and posteriorly to lie against the posteromedial chest wall. The stomach appears pinched
lies in the chest. Note that it has “fallen” medially and posteriorly to lie against the posteromedial chest wall. The stomach appears pinched  as it traverses the defect in the diaphragm (collar sign).
as it traverses the defect in the diaphragm (collar sign).
 directly abuts the lung, and is not confined by the diaphragm.
directly abuts the lung, and is not confined by the diaphragm.
 extending upward through a diaphragmatic defect.
extending upward through a diaphragmatic defect.










 Discontinuity of hemidiaphragm with focal defect (segmental diaphragmatic defect)
Discontinuity of hemidiaphragm with focal defect (segmental diaphragmatic defect) Dangling diaphragm sign: Free edge of torn diaphragm curls inward on axial images rather than continuing its normal course parallel to chest wall
Dangling diaphragm sign: Free edge of torn diaphragm curls inward on axial images rather than continuing its normal course parallel to chest wall Absent diaphragm sign: Absence of diaphragm in expected location (without visualization of discrete tear)
Absent diaphragm sign: Absence of diaphragm in expected location (without visualization of discrete tear) Fallen or dependent viscus sign: Herniated viscus abuts posterior ribs and thoracic wall without intervening lung
Fallen or dependent viscus sign: Herniated viscus abuts posterior ribs and thoracic wall without intervening lung






 Radiographs are significantly less sensitive than CT for diaphragmatic injury, but may often be initial study performed
Radiographs are significantly less sensitive than CT for diaphragmatic injury, but may often be initial study performed





