Chronic: Small adrenals with dots of calcification and low signal on all MR sequences
• Renal tuberculosis
Most common CT finding is renal calcification (50%)
Papillary necrosis is a very common early finding
Focal wedge-shaped hypodense areas, small hypodense nodules, or discrete renal abscess
Urothelial thickening, caseous debris, and strictures of calyces and infundibuli may lead to hydronephrosis
• Hepatosplenic tuberculosis
Hepatosplenomegaly with hypodense nodules of variable size
CLINICAL ISSUES
• Often presents with fever, weight loss, and abdominal pain
• May or may not have evidence of pulmonary TB
Negative chest radiograph or negative tuberculin skin test does not exclude extrapulmonary TB
(Left) Axial CECT in an asymptomatic elderly man shows calcification of mesenteric nodes usually seen in elderly individuals who have had exposure to enteric mycobacteria, often from drinking unpasteurized milk.
(Right) Axial CECT in a liver transplant recipient shows marked thickening of the omentum , peritoneum, and mesentery, with enlargement of mesenteric nodes . Loculated ascites was also present (not shown). This patient’s reactivated TB with TB peritonitis was first acquired in his native country.
(Left) Spot film from a small bowel follow-through in a 25-year-old immigrant from India shows deformity of the terminal ileum and cecum , with asymmetric thickening and stiffening of the bowel walls, ultimately found to represent TB.
(Right) Coronal CECT in an immigrant patient demonstrates asymmetric thickening of the cecum, which has a cone-shaped appearance in a patient with tuberculous colitis.
TERMINOLOGY
Abbreviations
• Tuberculosis (TB)
Definitions
• Infection by Mycobacterium tuberculosis
IMAGING
General Features
• Best diagnostic clue
Most common sites of involvement in abdomen are lymph nodes, GU tract, peritoneum, and GI tract
– Abdominal lymphadenopathy most common (2/3 cases)
– GU tract is most common organ system involved
– Any abdominal/pelvic organ or structure may be involved
Liver, spleen, biliary tree, pancreas, and adrenal glands unusual and more likely in HIV patients or patients with miliary TB
Imaging Recommendations
• Best imaging tool
CECT
Radiographic Findings
• Often no evidence of lung disease (CXR or CT can be normal)
• Lymphadenopathy (tuberculous lymphadenitis)
Can range from increased number of normal-sized nodes to massively enlarged conglomerate nodal masses
– Mesenteric and peripancreatic lymph nodes most commonly involved
– Multiple groups often affected simultaneously
Enlarged, necrotic nodes with hypoattenuating centers and hyperattenuating enhancing rims on CT (40-60%)
– Characteristic of caseous necrosis
– Mixed attenuation nodes are also possible
Nodes calcify with healing: TB probably most common cause of mesenteric nodal calcification
• Tuberculosis peritonitis
3 imaging patterns: Wet, dry, and fibrotic fixed
– Wet type: Large amount of free or loculated ascites
Higher than water density due to protein/cellular content
Complex ascites with septations or fibrinous strands
– Dry type: Mesenteric and omental thickening, fibrous adhesions, and caseous nodules
– Fibrotic fixed: Discrete masses in omentum with matted loops of bowel ± loculated ascites
CT is ∼ 69% sensitive for TB peritonitis
– Difficult to distinguish from carcinomatosis
– Carcinomatosis more likely to demonstrate discrete implants or omental caking
• Gastrointestinal tuberculosis
Ileocecal region affected in 90% of cases
– Common site due to presence of lymph tissue and stasis of bowel contents in that location
– Cecum and terminal ileum are usually contracted (cone-shaped cecum) with asymmetric wall thickening of ileocecal valve and medial cecum
Ileocecal valve is “gaping”
– Strictures, regional inflammation common
– Regional lymphadenopathy with central caseation
Involvement of stomach and proximal small bowel is rare
– Stomach: Affects antrum and distal body, often simulating peptic ulcer disease
– Duodenum: Wall thickening and luminal narrowing
– Any portion of GI tract can be theoretically involved
• Hepatosplenic tuberculosis
Micronodular pattern
– Innumerable 0.5–2.0 mm nodules may or may not be discretely visualized (most often hypodense on CT and hyperechoic on US)
Only gold members can continue reading. Log In or Register to continue














 usually seen in elderly individuals who have had exposure to enteric mycobacteria, often from drinking unpasteurized milk.
usually seen in elderly individuals who have had exposure to enteric mycobacteria, often from drinking unpasteurized milk.
 , peritoneum, and mesentery, with enlargement of mesenteric nodes
, peritoneum, and mesentery, with enlargement of mesenteric nodes  . Loculated ascites was also present (not shown). This patient’s reactivated TB with TB peritonitis was first acquired in his native country.
. Loculated ascites was also present (not shown). This patient’s reactivated TB with TB peritonitis was first acquired in his native country.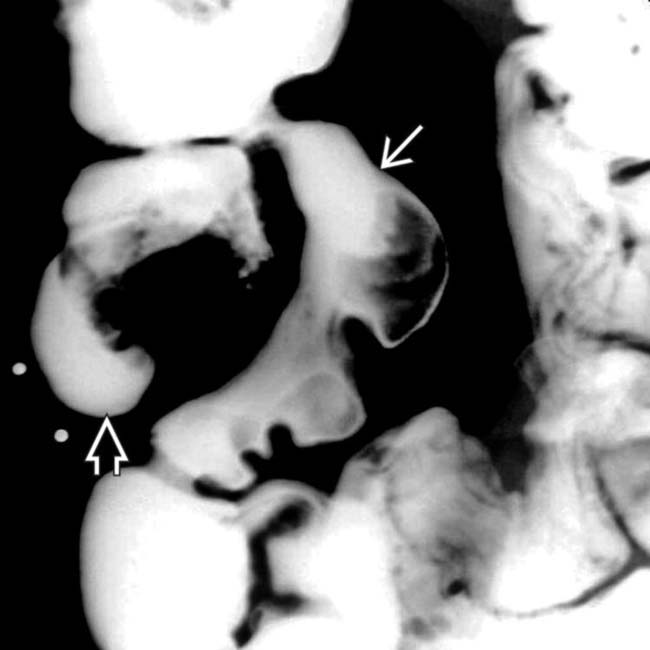
 and cecum
and cecum  , with asymmetric thickening and stiffening of the bowel walls, ultimately found to represent TB.
, with asymmetric thickening and stiffening of the bowel walls, ultimately found to represent TB.
 of the cecum, which has a cone-shaped appearance in a patient with tuberculous colitis.
of the cecum, which has a cone-shaped appearance in a patient with tuberculous colitis.


 Can range from increased number of normal-sized nodes to massively enlarged conglomerate nodal masses
Can range from increased number of normal-sized nodes to massively enlarged conglomerate nodal masses Enlarged, necrotic nodes with hypoattenuating centers and hyperattenuating enhancing rims on CT (40-60%)
Enlarged, necrotic nodes with hypoattenuating centers and hyperattenuating enhancing rims on CT (40-60%)
 3 imaging patterns: Wet, dry, and fibrotic fixed
3 imaging patterns: Wet, dry, and fibrotic fixed


 Ileocecal region affected in 90% of cases
Ileocecal region affected in 90% of cases

 Micronodular pattern
Micronodular pattern




