George M. Bridgeforth and Mark Nolden
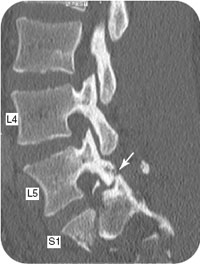
A 19-year-old man was an unrestrained backseat passenger in an automobile involved in a collision with another motor vehicle. he now presents with left sacral and left groin pain.
CLINICAL POINTS
- Common causes of unilateral facet dislocations are motor vehicle accidents and contact sports injuries.
- Radiculopathy occurs on the side of the unilateral facet dislocation.
- Some patients with radiculopathies present with diminished sensation of the fingers.
- These types of dislocations may be associated with a traumatic brain injury.
Clinical Presentation
The most common cause of unilateral facet injuries are motor vehicle accidents, followed by contact sports injuries. The mechanism of injury involved in this spinal injury is flexion/rotation. Unlike bilateral facet injuries, most unilateral facet injuries are stable and occur in the midcervical region. Facet injuries to the lumbar spine are less common and are more likely to be associated with spinal
fractures. However, the unilateral cervical facet injuries may also be associated with facet fractures. Therefore, all patients should be stabilized on a spine board with a hard collar. Instability should always be assumed until proven otherwise.
The most common clinical presentation with a unilateral facet dislocation is radicular cervical pain. The flexion rotation injury causes the superior facet to slide over the inferior facet. The inferior facet is forced caudally and cause nerve root impingement of the neuroforamen beneath the inferior facet. This bony impingement where the nerve root exists from the vertebral column produces radicular symptoms. In selected cases, there may an accompanying disc protrusion as well.
Patients with C5 (fifth cervical nerve root irritation) have pain and numbness that radiates to the deltoid region (outside of the shoulder). Differential diagnosis includes C5 radiculopathies from disc herniations without facet dislocations as well as such shoulder injuries as acute humeral head, upper shaft fractures, humeral dislocations, and acute rotator cuff tears. A facet dislocation may be misdiagnosed as an acute shoulder injury or a herniated cervical disc. A thorough musculoskeletal examination followed by radiological studies can be very helpful.
Patients with C5 radiculopathies from unilateral facet dislocations of herniated discs usually demonstrate decreased sensation along the lateral deltoid (outside of the shoulder at the head of the humerus) to pinprick. In the acute setting following a cervical injury, it is not advised to assess cervical range of motion until an unstable spinal injury has been ruled out. Patients with acute radiculopathies from herniated discs often have impaired cervical range of motion as well. Later findings with severe radiculopathies from unilateral facet dislocations or herniated discs include biceps weakness (weak elbow flexion with the handheld palm facing upward) on the affected side and a diminished or absent biceps (C5) reflex.
C6 radiculopathies from unilateral facet dislocations or cervical herniations lead to pain and/or numbness that radiates to the thumb and index finger (Hoppenfeld six shooter). Later stages may manifest weakness with wrist extension (C6–C7 muscle function) and a diminished or absent brachioradial reflex (C6) at the wrist is very helpful. C7 radiculopathies have numbness that radiates to the middle finger. Marked nerve root involvement may present with weakness of grip strength and triceps function (weak elbow extension). Additional findings may include diminished or absent triceps reflex on the affected side. Early radiculopathies have deceased sensation of the middle finger. Marked nerve root involvement present with weakness of wrist flexion as well. C8 injuries radiate to the little finger. Early radiculopathies present with diminished sensation of the little finger.
Patients with cervical (or lumbar) stenosis usually present with bilateral radiculopathies affecting both upper extremities. In addition, there may involvement affecting more than one spinal level. Radiographs show narrowed foramen (exit canals for the spinal nerves) on the lateral radiographs and on the oblique radiographs.
With all acute cervical injuries, it is imperative that the examiner evaluates the lower extremities for upper motor neuron signs. Most nerve root injuries are lower motor neuron injuries. Lower motor neuron injuries are characterized by sensory loss, motor weakness, hyporeflexia, or areflexia (diminished or absent) reflexes. On the other hand, upper motor neuron injuries involve damage to the central nervous system (brain or spinal cord).
Unlike lower motor neuron injuries, upper motor neuron injuries are characterized by weakness, hyperactive reflexes, upgoing plantar responses (positive Babinski reflexes in the feet), clonus (recurrent jerking reflexes), and clasp-knife spasticity (increased muscle tone that eventually yields to marked resistance applied by an examiner across a joint). Patients with cervical injuries who have bilateral upper motor neuron signs affecting the lower extremities have either accompanying acute cervical spinal cord injuries or severe bilateral head injuries. With acute cervical injuries, this should prompt further evaluation with computed tomography (CT) of the head and the cervical spine.
PATIENT ASSESSMENT 
- Look for nerve root impingement with radicular symptoms secondary to a locked dislocated facet.
- Most unilateral facet dislocations are stable. However, always assume instability until proven otherwise.
- Rule out associated head, shoulder, and thoracic trauma, especially with cervical injuries.
- Check for nerve root irritation (i.e., pinched nerve) at the site of the injury.
- Always check neurovascular status carefully.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


