George M. Bridgeforth and George Holmes
A 33-year-old woman fell down the stairs. She presents with a gross deformity of the left foot.

CLINICAL POINTS
- Lisfranc injuries vary in severity from sprains to fractures/dislocations.
- These injuries are difficult to diagnose.
- The neurovascular status of all patients should be checked carefully.
Clinical Presentation
A Lisfranc injury is damage to the joints in the midfoot—the Lisfranc joint, or tarsometatarsal articulation of the foot. The most common mechanism of injury is torsion/impaction against the plantar flexed foot (i.e., foot is pointed downward). Common examples would include being involved in a motor vehicle accident or forklift accident, when the foot gets caught under a brake. Another example would be having the foot caught on the rung of a ladder or falling down the stairs (with the foot in a plantar flexed position). However, Lisfranc injures may be also be caused by axial loads (heavy items) that land directly on the dorsal foot.
Lisfranc injuries are rare but are associated with a high risk of chronic secondary disability. They are easily missed during the initial evaluation, and the best way to detect these injuries is to have a high index of suspicion. Normal radiographs do not rule out an associated Lisfranc injury. Valuable clinic clues include marked pain, swelling, and tenderness over the midfoot, especially over the tarsometatarsal joint; some inability to bear weight; and limited range of motion. The presence of these signs and symptoms and a lack of any improvement may point to a Lisfranc injury.
PATIENT ASSESSMENT 
- Marked pain, swelling, and tenderness over the midfoot
- Pain-limited weight bearing and range of motion
NOT TO BE MISSED 
- Foot fracture
- Foot contusion
- Osteomyelitis (especially in patients with diabetes)
Radiolographic Evaluation
Anteroposterior (AP), lateral, and oblique views of the foot should be obtained. Radiographs are helpful but are not always diagnostic. If a Lisfranc injury is suspected but radiographs show only soft tissue swelling, a computed tomography scan or a magnetic resonance imaging scan may be necessary (Fig. 27.1).
Basically, there are two types of Lisfranc injuries: homolateral and divergent.
HOMOLATERAL LISFRANC INJURY
With a homolateral Lisfranc injury (Fig. 27.2), all of the metatarsal fractures are pointing in the same direction. There is marked lateral displacement of the forefoot at the Lisfranc (tarsometatarsal) joint on the AP view. On the lateral view, there is a pronounced step-off between the cuboid–cuneiforms and the proximal metatarsals (at the Lisfranc joint). Although Lisfranc injuries are one of the most common injuries of the foot, they are frequently missed. Large fracture dislocations are easy to identify.
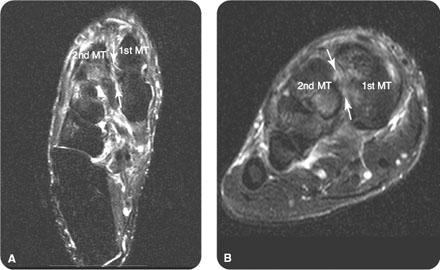
FIGURE 27.1 Lisfranc ligament injury. Selected (A) oblique and (B) coronal T2-weighted, fat-saturated images from magnetic resonance imaging scan of the right foot after a twisting injury in a 43-year-old man. Abnormal increased fluid signal is demonstrated in the Lisfranc ligament (arrows).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


