George M. Bridgeforth and John Cherf
A 21-year-old woman complains of right knee pain, which began after she fell on the sidewalk 1 month ago.
CLINICAL POINTS
- Most dislocations are lateral.
- Patients have an antalgic gait.
- Patients with ruptured quadriceps or patella tendons have knee effusions with an inability to extend the knee against gravity.
Clinical Presentation
Most patella dislocations are characterized by pain, swelling, and limited weight-bearing. Patients may complain of a “pop,” with the knee “popping back into place.” There may be mild to moderate swelling. Usually, there is no associated erythema, and the knee is not warm. However, pain-limited range of motion may be present, and the patient may exhibit an antalgic gait (pronounced limp).
Most patella, dislocations occur when the kneecap comes completely out of its groove and rests on the outside of the knee joint. The mechanism of injury is a twisting action. This injury common, particularly in adolescent girls and athletes. Sports frequently associated with patella dislocation include soccer, gymnastics, and ice hockey.
When the kneecap goes “out of joint” the first time, ligaments that normally hold the kneecap in position are torn. The structure most often torn is the medial patellofemoral ligament. This ligament secures the patella to the inside (medial) of the knee. When a patella dislocation occurs, the medial patellofemoral ligament is damaged and allows the kneecap to move out of the groove (Fig. 14.1). Once this ligament is torn, it often does not heal properly, and the patella can then dislocate more easily, which is why patella dislocation recurs in some patients with this ligament injury. It should be noted that some subluxations might not be as apparent on examination.
A useful sign for dislocated patella is the presence of patella apprehension. The knee is placed into slight flexion, and both hands are placed across the patella with both thumbs placed on the medial side of the patella. The patella is slowly pushed laterally by the examiner’s thumbs. Patients with a patella instability views (barring an acute fracture) complain of pain and apprehension. In response, they try to straighten the knee, which locks the knee preventing further displacement.
Radiographic Evaluation
It is necessary to order anteroposterior (AP), lateral. Optional radiographs include the following:
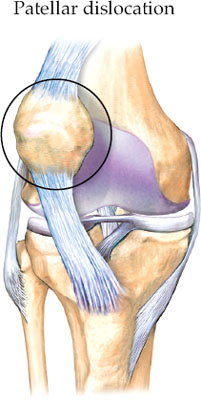
FIGURE 14.1 Right knee with a lateral patellar dislocation. Note the intact medial and lateral collateral ligaments as well as the intact quadriceps and patellar tendons. (Asset provided by Anatomical Chart Co.)
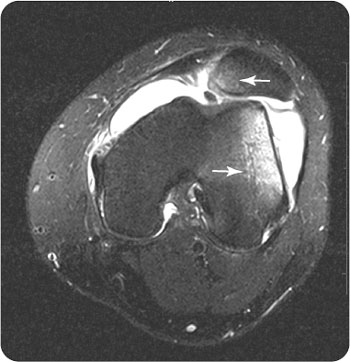
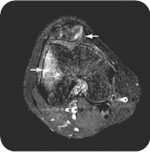
FIGURE 14.2 An axial T2-weighted image through the left knee of an 18-year-old male rugby player who injured his knee during a match. Demonstrated is a bone marrow edema pattern consistent with transient lateral patellar dislocation-relocation. There is an extensive knee joint effusion with an associated tearing of the anteromedial retinaculum/capsule resulting in lateral positioning of the patella. There is a shallow trochlear groove.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


