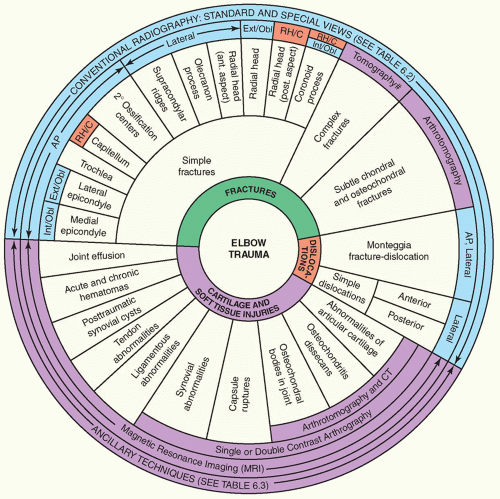
Trauma to the elbow is commonly encountered in all age groups but is particularly common in childhood when children, as toddlers, often sustain elbow injuries. Play and athletic activities in childhood and young adolescence are also frequent occasions of trauma. Although history and clinical examination usually provide clues to the correct diagnosis, radiologic examination is indispensable in determining the type of fracture or dislocation, the direction of the fracture line and the position of the fragments, and also in evaluating concomitant soft-tissue injuries.
Anatomic-Radiologic Considerations
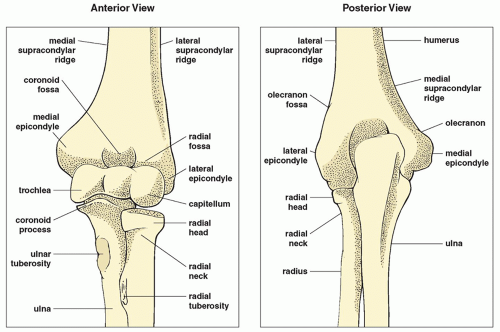
The elbow articulation, a compound synovial joint, comprises the humeroulnar (ulnatrochlear), the humeroradial (radiocapitellar), and the proximal radioulnar joints (
Fig. 6.1). It is a hinged articulation with approximately 150 degrees of flexion from a completely extended position. The flexion and extension movements in the elbow occur in the ulnatrochlear and radiocapitellar joints. The biceps, brachioradialis, and brachialis muscles are the primary elbow flexors, while the triceps is the extensor of the elbow joint (
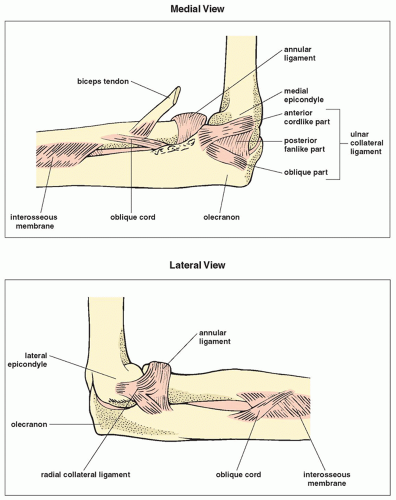
Fig. 6.2). Rotational movement occurs as the head of the radius, held tightly by the annular ligament of the ulna, rotates within the ulna’s radial notch. The proximal and distal radioulnar joints allow 90 degrees of pronation and supination of the forearm. The stability of the joint is ascertained by the group of ulnar collateral ligaments (UCLs) medially and radial collateral ligaments laterally (
Fig. 6.3). The UCL consists of the anterior bundle, which extends from the anteroinferior aspect of the medial epicondyle to the medial coronoid margin; the posterior bundle, which extends from the posteroinferior aspect of the medial epicondyle to the medial olecranon margin; and the transverse bundle, which extends over the notch between the coronoid process and the olecranon. The radial collateral ligament is thinner than the UCL and inserts in the annular ligament, which in turn encircles the radial head and attaches to the anterior and posterior margins of the radial notch of the ulna. A fibrous capsule deep within the ligament structures surrounds the elbow joint. The anterior joint capsule and synovium insert proximally to the coronoid and radial fossae at the anterior aspect of the humerus. The posterior joint capsule attaches to the humerus just proximal to the olecranon fossa.
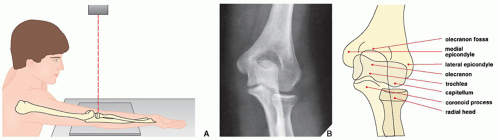
When trauma to the elbow is suspected, radiographs are routinely obtained in the anteroposterior and lateral projections, occasionally supplemented by internal and external oblique views.
The
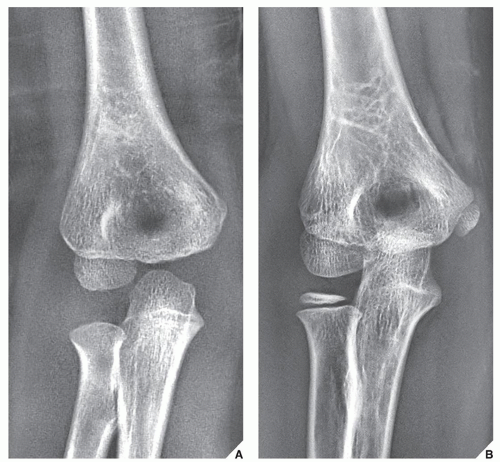
anteroposterior projection usually suffices to demonstrate an injury to the medial and the lateral epicondyles, the olecranon fossa, the capitellum, the trochlea, and the radial head (
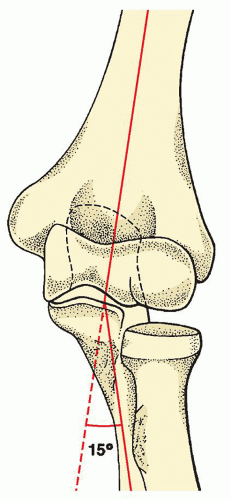
Fig. 6.4). It also reveals an important anatomic relation of the forearm to the central axis of the arm known as the
carrying angle (
Fig. 6.5). Normally, the long axis of the forearm forms a valgus angle of 15 degrees with the long axis of the arm; the forearm is thus angled laterally, that is, away from the central axis of the body.
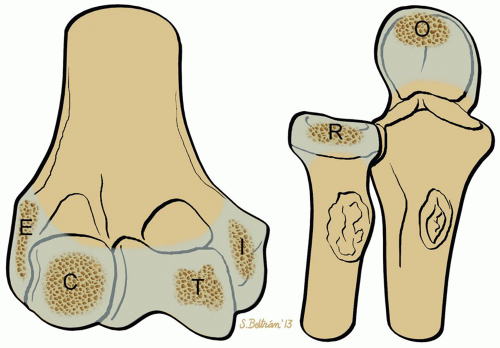
On the anteroposterior view in children, it is essential to recognize the four secondary ossification centers of the distal humerus: those of the capitellum, the medial and the lateral epicondyles, and the trochlea. The usual order in which these centers appear and the age at which they become radiographically visible are important factors in the evaluation of injuries to the elbow (
Fig. 6.6). The displacement of any of these centers serves as a diagnostic indicator of the type of fracture or dislocation. For example, the medial epicondyle always ossifies before the trochlea. If radiographic examination in a child between the age of 4 and 8 years reveals a bony structure in the region of the trochlea (i.e., before this center of ossification should appear) and shows no evidence of the ossification center of the medial epicondyle, then it must be assumed that the ossification center of the medial epicondyle has been avulsed and displaced into the joint (
Fig. 6.7). Some radiologists prefer to use a mnemonic “CRITOE 1-3-5-7-9-11” to determine the sequence and age of appearance of the six ossification centers around elbow joint: the capitellum, the radial head, the internal (medial) epicondyle, the trochlea, the olecranon, and the external (lateral) epicondyle (
Figs. 6.8 and
6.9).
The
lateral view of the elbow allows sufficient evaluation of the olecranon process, the anterior aspect of the radial head, and the humeroradial articulation. It is limited, however, in the information it can provide, particularly with respect to the posterior half of the radial head and the coronoid process, because of the overlap of osseous structures (
Fig. 6.10).
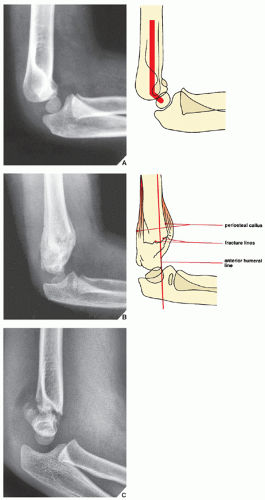
As with the anteroposterior projection, the lateral view in children reveals significant configurations and relations, which, if distorted, indicate the presence of an abnormality. The distal humerus in children has an angular appearance resembling a hockey stick, the angle of which normally measures approximately 140 degrees. Loss of this configuration occurs in supracondylar fracture (
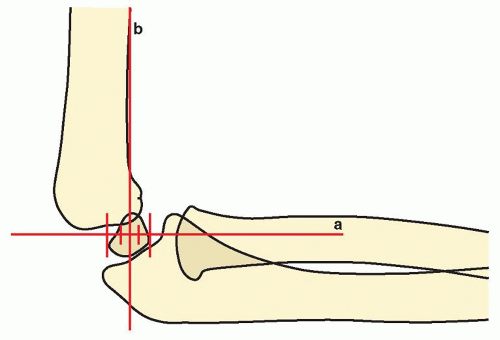
Fig. 6.11). Rogers has pointed out, in addition, the importance of the position of the capitellum relative to the distal humerus and the proximal radius. He found that a line drawn along the longitudinal axis of the proximal radius passes through the center of the capitellum and that a line drawn along the anterior cortex of the distal humerus and extended downward through the articulation intersects the middle third of the capitellum (
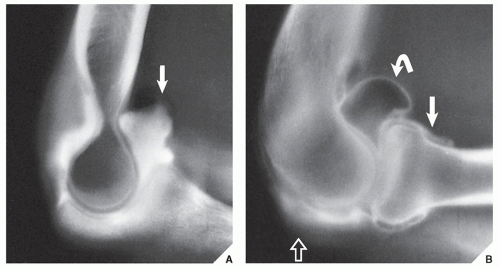
Fig. 6.12). A disruption of this relation serves as an important indication of the possible presence of a fracture or dislocation. Finally, regardless of the patient’s age, a displacement of the normal positions of the fat pads of the elbow also provides a useful diagnostic clue to
the presence of a fracture. Normally, the posterior fat pad, which lies deep in the olecranon fossa, is not visible on the lateral view. When it becomes visible and the anterior fat pad appears displaced—the positive fat-pad sign (
Fig. 6.13; see also
Figs. 6.27B and
6.32A)—demonstration of the fracture line should be undertaken.
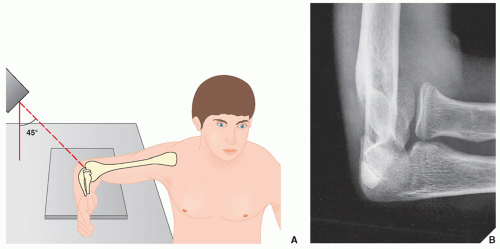
The
radial head-capitellum view is a variant of the lateral projection, which was introduced by Greenspan in 1982. As it overcomes the major limitation of the standard lateral view by projecting the radial head ventrad, free of overlap by the coronoid process, it has proved to be a particularly effective technique. In addition to the radial head, it also clearly demonstrates the capitellum, the coronoid process, the humeroradial and humeroulnar articulations (
Fig. 6.14), and subtle fractures of these structures that may be obscure on other projections (see
Figs. 6.29,
6.30, and
6.36).
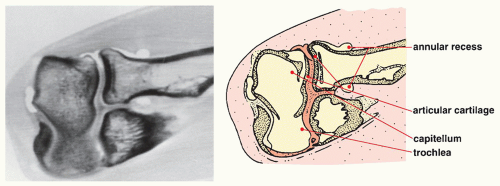
Other modalities may also be necessary for sufficient evaluation of an injury to the elbow. Single-contrast or, preferably, double-contrast arthrography, combined (in the past) with tomography (
arthrotomography) and presently with computed tomography (CT), has proved effective in visualizing subtle chondral fractures, osteochondritis dissecans, synovial and capsular abnormalities, and osteochondral bodies in the joint. In general, indications for elbow arthrography include detection of the presence, size, and number of intraarticular osteochondral bodies; determination of whether calcifications around the elbow joint are intraarticular or extraarticular; evaluation of the articular cartilage; evaluation of juxtaarticular cysts if they are communicating with the joint; evaluation of the joint capacity; and evaluation of various synovial and capsular abnormalities. Singlecontrast arthrography is preferable when evaluating synovial abnormalities and intraarticular osteochondral bodies because double contrast may result in air bubbles in the joint. Double-contrast arthrography, however, provides more detailed information; in particular, the articular surface and synovial lining are better delineated and the small details can be better visualized (
Fig. 6.15). In the past, in conjunction with elbow arthrography, conventional tomography was used in a procedure called
arthrotomography (
Fig. 6.16); however, currently it has been substituted by CT examination (CT-arthrography) (
Fig. 6.17).
Axial CT images of the extended elbow are occasionally effective in demonstrating traumatic abnormalities. They are, however, difficult to obtain in the traumatized patient, and except for the visualization of the proximal radioulnar joint and ulnatrochlear articulation, they are not frequently used. Occasionally, these sections can demonstrate osteochondral fractures of the radial head and assess the integrity of the proximal radioulnar joint. However, Franklin and colleagues noted that axial CT images of the flexed elbow (so-called coronal sections) provide an ideal plane for the evaluation of the olecranon fossa and the space between the trochlea and the olecranon process posteriorly, as well as the radius and the capitellum, and the trochlea and the coronoid process anteriorly. Axial scans through the flexed elbow also allow additional demonstration of the proximal radius in its long axis.
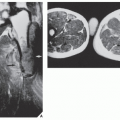
Magnetic resonance imaging (MRI) examination effectively demonstrates traumatic abnormalities of the elbow joint and surrounding soft tissues. Axial, sagittal, and coronal planes are routinely used for elbow imaging. The axial plane is ideal to display the anatomic relationship of the proximal radioulnar joint and the head of the radius. Various tendons, muscles, annular ligament, and neurovascular bundles are also effectively imaged. On coronal images, the trochlea, capitellum, and radial head are well demonstrated, as well as the various tendons, ligaments, and muscles around the elbow (
Fig. 6.18A). On the sagittal images, the ulnatrochlear and radiocapitellar articulations are well seen, and the biceps, triceps, and brachialis muscle groups are well demonstrated in their long axis. The biceps tendon and anconeus muscles are also well imaged (
Fig. 6.18B,C).
MR arthrography (MRa) is occasionally performed, mainly to evaluate synovial abnormalities and integrity of the joint capsule and ligaments. In addition, subtle intraarticular loose bodies can be detected with this technique, and the stability of osteochondral fracture or osteochondritis dissecans of the capitellum can be assessed. Similar to one used for shoulder MRa, a concentration of gadolinium mixed with normal saline, iodinated contrast agent, and lidocaine is prepared and a total of up to 10 mL of fluid is injected into the elbow joint. Lateral approach, identical to the technique for conventional elbow arthrography (see
Fig. 6.16), is preferred. Coronal, sagittal, and axial images are obtained using fat-suppressed spin echo sequences (
Fig. 6.19). During the evaluation of MRI of the elbow, it is helpful to use a checklist as provided in
Table 6.1.










 Radiologic Evaluation of Skeletal Anomalies
Radiologic Evaluation of Skeletal Anomalies
 Inflammatory Arthritides
Inflammatory Arthritides
 Benign Tumors and Tumor-like Lesions II: Lesions of Cartilaginous Origin
Benign Tumors and Tumor-like Lesions II: Lesions of Cartilaginous Origin
 Benign Tumors and Tumor-Like Lesions III: Fibrous, Fibroosseous, and Fibrohistiocytic Lesions
Benign Tumors and Tumor-Like Lesions III: Fibrous, Fibroosseous, and Fibrohistiocytic Lesions
 Benign Tumors and Tumor-Like Lesions IV: Miscellaneous Lesions
Benign Tumors and Tumor-Like Lesions IV: Miscellaneous Lesions
 Upper Limb III: Distal Forearm, Wrist, and Hand
Upper Limb III: Distal Forearm, Wrist, and Hand



