Urinary Tract and Adrenal Glands
QUESTIONS
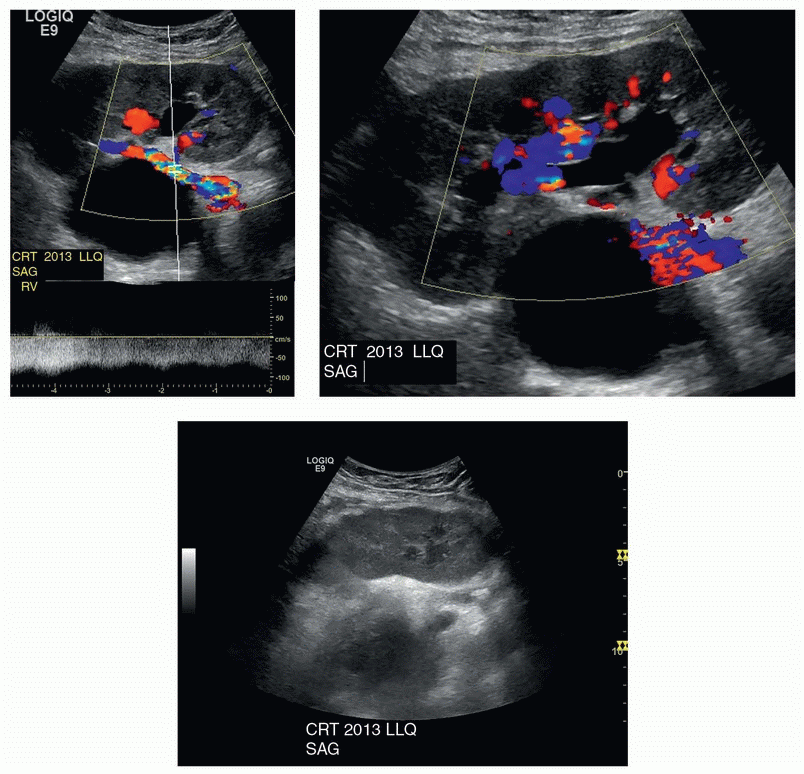
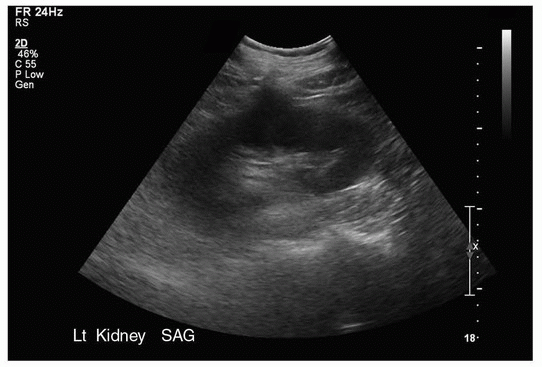
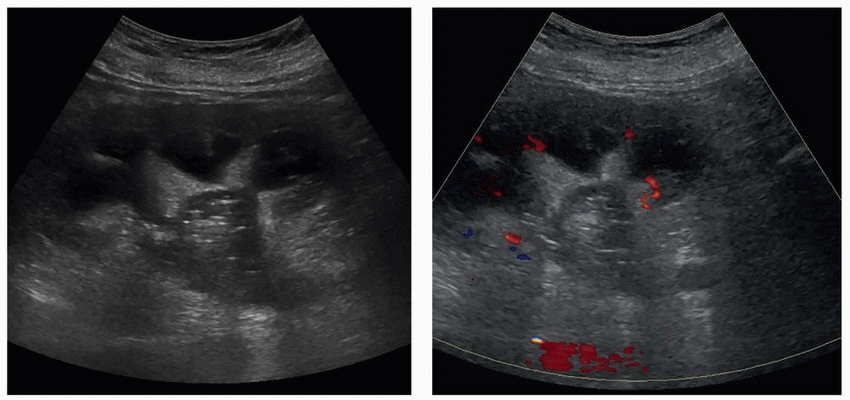
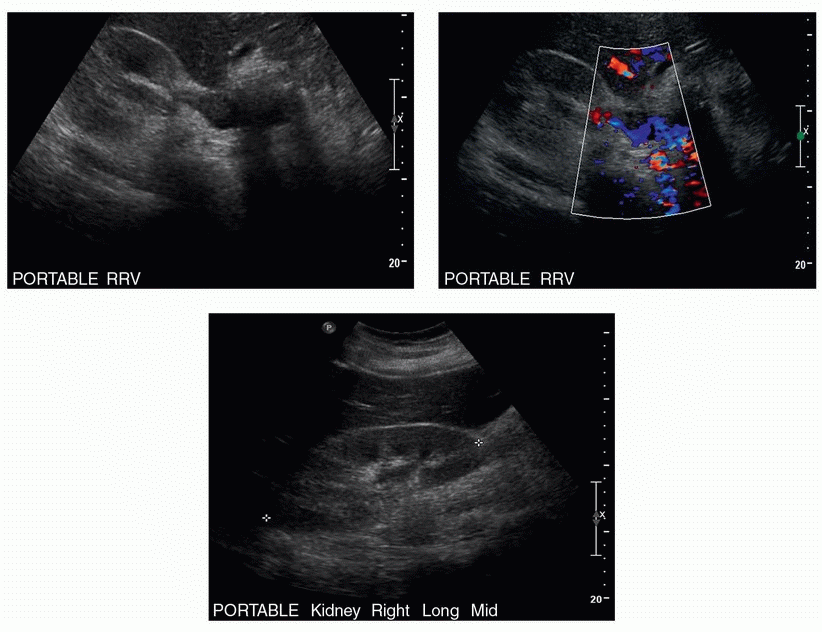
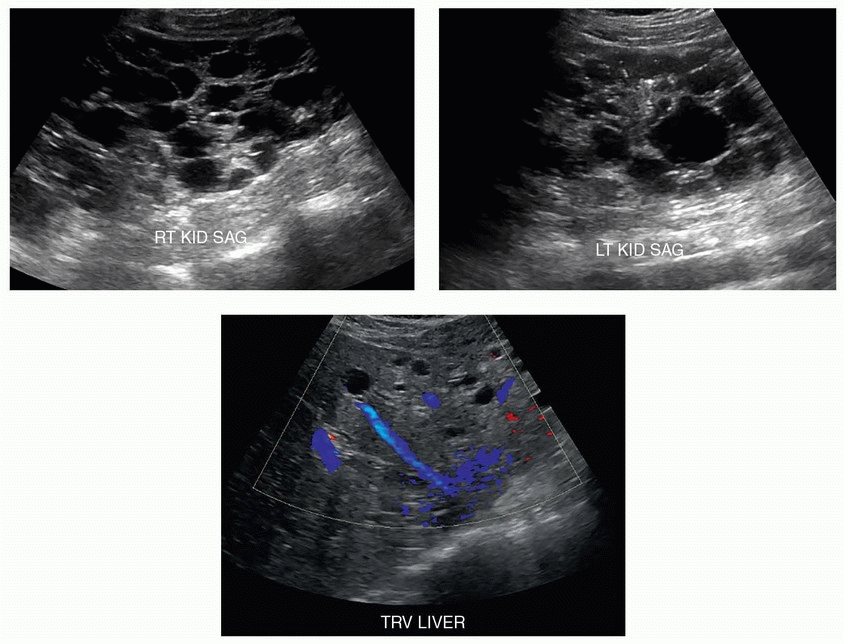
1 A 26-year-old female with renal failure underwent renal ultrasound. What is the most common cause of the finding shown in the images?
|
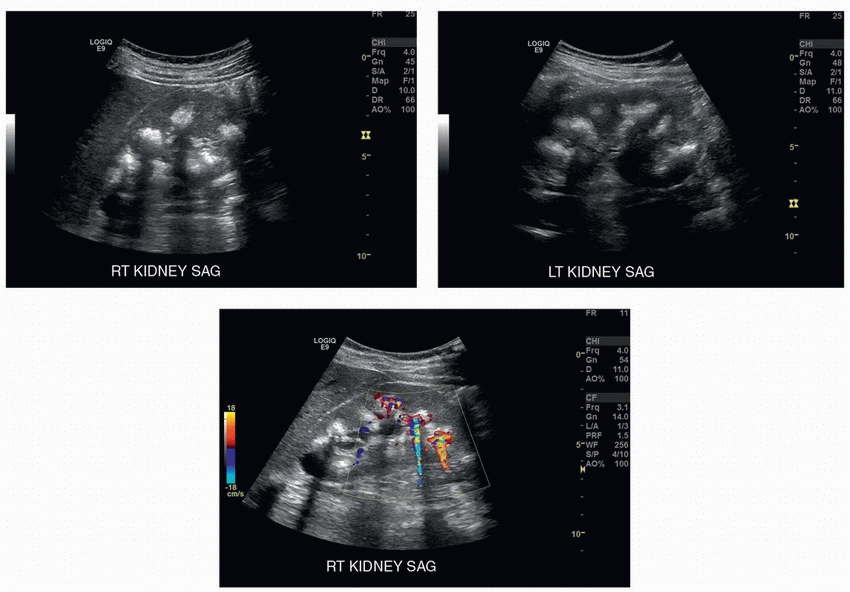
A. Medullary sponge kidney
B. Renal tubular acidosis type I
C. Primary hyperparathyroidism
D. Chronic glomerulonephritis
E. Hypervitaminosis D
View Answer
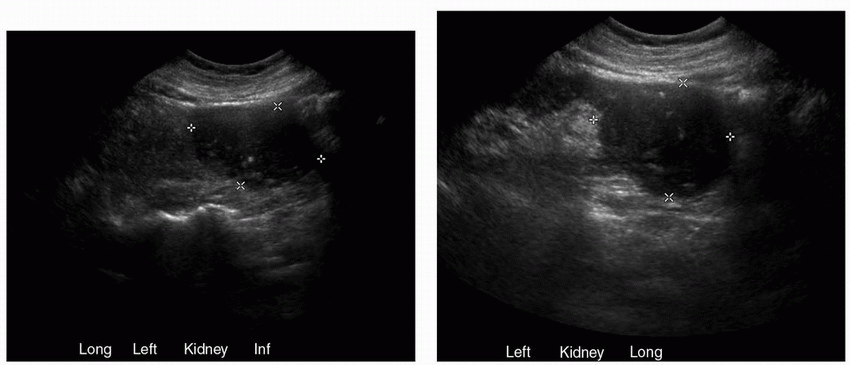
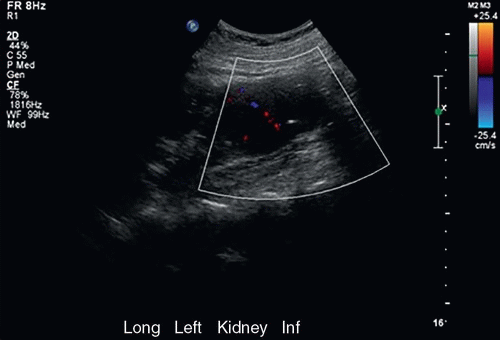
1 Answer C. Sagittal images of both kidneys show generalized increased echogenicity of the renal pyramids and associated posterior acoustic shadowing, consistent with calcium deposition. Color Doppler image of the right kidney shows “twinkle” artifact from the renal calcifications. The findings are consistent with medullary nephrocalcinosis. The common causes of medullary nephrocalcinosis in the order of frequency are as follows: 40%, primary hyperparathyroidism; 20%, renal tubular acidosis type I; and 20%, medullary sponge kidney. Other causes such as hypervitaminosis D states and milk-alkali syndrome are less common. Chronic glomerulonephritis results in cortical nephrocalcinosis (and not medullary nephrocalcinosis).
References: Hertzberg BS, Middleton WD. Ultrasound: the requisites, 3rd ed. Philadelphia, PA: Elsevier, 2016:130-131.
Rumack CM, Wilson SR, Charboneau WJ. Diagnostic ultrasound, 4th ed. Philadelphia, PA: Elsevier Health Sciences, 2011:346-348.
2a A 66-year-old male presents with hematuria. Ultrasound images of the midline pelvis are shown. Which of the following is the most likely diagnosis?
|
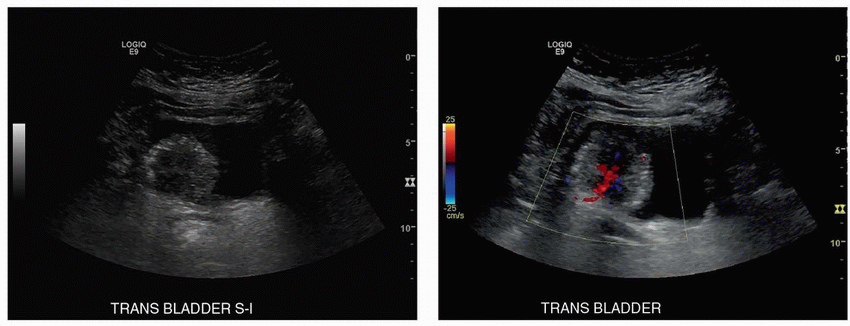
A. Bladder cancer
B. Fungus ball
C. Blood clot
D. Bladder stone
View Answer
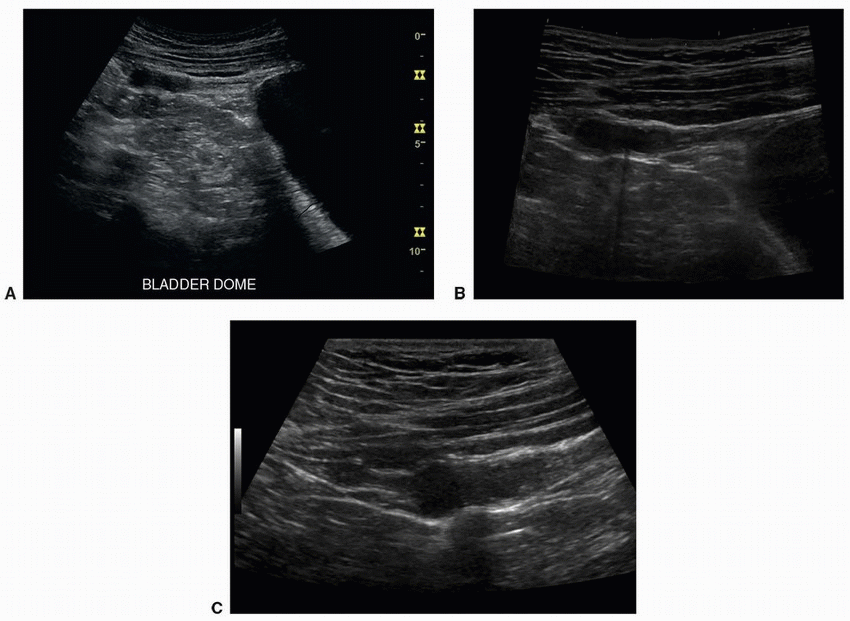
2a Answer A. Bladder cancer is usually seen as a sessile or pedunculated mass projecting into the bladder lumen. Immobility and presence of internal vascularity are useful distinguishing features. Fungus balls and blood clots are mobile masses without vascularity. Bladder stones are mobile and echogenic and show posterior acoustic shadowing.
2b Which of the following is the most common type of bladder cancer?
A. Adenocarcinoma
B. Transitional cell carcinoma
C. Squamous cell carcinoma
D. Neuroendocrine carcinoma
View Answer
2b Answer B. Approximately 90% of bladder tumors are transitional cell carcinoma (TCC). The majority of TCC arise at the trigone and along the lateral and posterior bladder walls. Squamous cell carcinomas account for 5% to 8% of all bladder tumors. Adenocarcinoma of the bladder is rare (˜2% of all bladder tumors) and tends to occur in urachal remnants and in bladder exstrophy. Neuroendocrine (small cell) tumor of the bladder is rarer, accounting for <0.5% of all bladder neoplasms.
2c Which of the following is the most important risk factor for bladder cancer in the United States?
A. Smoking
B. Calculus
C. Recurrent urinary tract infections
D. Chemical carcinogens
View Answer
2c Answer A. The pathogenesis for urothelial tumors is direct prolonged contact of the bladder urothelium with urine containing excreted carcinogens. The most well-established risk factor for bladder cancer is cigarette smoking. Cigarette smoking accounts for one-third to one-half of all cases of bladder cancer. There is also a well-documented causal link between urothelial cancer and a variety of occupational and environmental chemicals such as aniline, benzidine, aromatic amines, and azo dyes. Therefore, occupational exposure to chemical carcinogens is the second most important risk factor after smoking, estimated to account for as much as 20% of all bladder cancer. Chronic irritation from bladder calculi and recurrent urinary tract infections is strongly associated with squamous cell carcinoma.
References: Hertzberg BS, Middleton WD. Ultrasound: the requisites, 3rd ed. Philadelphia, PA: Elsevier, 2016:167-168.
Rumack CM, Wilson SR, Charboneau WJ. Diagnostic ultrasound, 4th ed. Philadelphia, PA: Elsevier Health Sciences, 2011:359-360.
Wong-You-Cheong JJ, Woodward PJ, Manning MA, et al. Neoplasms of the urinary bladder: radiologic-pathologic correlation. Radiographics 2006;26:553-580.
3 A 32-year-old female receives an ultrasound as part of a routine obstetric workup and is found to have an abnormality adjacent to the left kidney. What is the most likely diagnosis from the following choices?
|
A. Adrenocortical carcinoma
B. Adrenal adenoma
C. Adrenal pseudocyst
D. Adrenal pheochromocytoma
View Answer
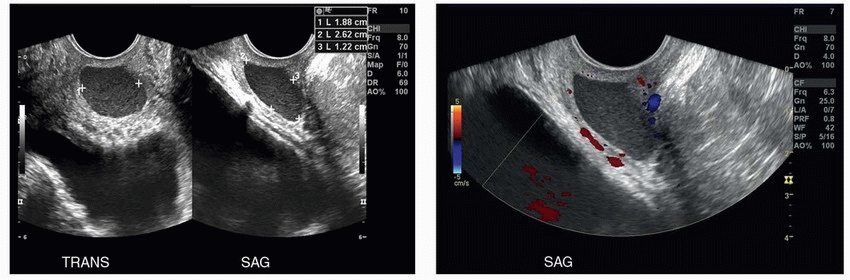
3 Answer C. A bilobed thin-walled anechoic adrenal lesion containing a thin septation with no internal color Doppler signal is shown. A thin smooth wall and lack of a solid component favors an adrenal cyst, pseudocyst, or parasitic cyst. Whereas true adrenal cysts are lined by endothelium, pseudocysts are surrounded by a fibrous capsule and are usually the sequelae of adrenal hemorrhage or infection. In addition, neoplasms including adrenocortical carcinoma, pheochromocytoma, and adenomas may undergo necrosis or degeneration leading to cystic components, which may be extensive especially in larger tumors. Careful inspection on contrast-enhanced CT or MRI should be performed to exclude a solid tumoral component. There have only been a few reported cases of entirely cystic pheochromocytoma.
References: Newhouse JH, Heffess CS, Wagner BJ, et al. Large degenerated adrenal adenomas: radiologic-pathologic correlation. Radiology 1999;210(2):385-391.
Lee TH, Slywotzky CM, Lavelle MT, et al. Best cases from the AFIP. Radiographics 2002;22(4):935-940.
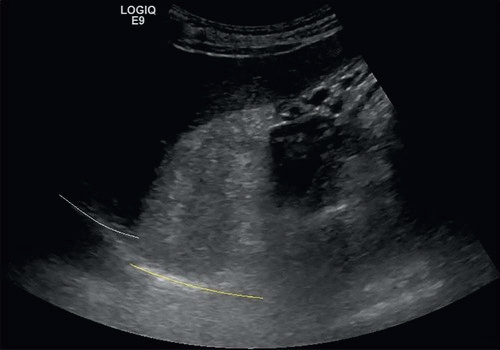
4a Imaging of the right flank was performed for flank pain in a 55-year-old male. What is the most likely explanation for the sonographic appearance of the suprarenal lesion?
|
A. Blood products
B. Bowel gas
C. Calcification
D. Fat
View Answer
4a Answer D. A large echogenic suprarenal mass is shown with associated impairment of acoustic penetration, indicating the presence of fat. Although gas can result in “dirty” acoustic shadowing, linear high-amplitude reflections are expected along the boundary closest to the probe. Blood products can have a variety of appearances but would not be expected to shadow. Large calcifications typically produce clean acoustic shadows.
4b Which of the following factors is expected to introduce uncertainty in measurement of this mass?
A. Speed of sound within the mass is higher than within the liver.
B. Speed of sound within the mass is lower than within the liver.
C. Speed of sound is equal within the mass and liver.
View Answer
4b Answer B. The average velocities of sound in fat and soft tissue are 1,450 and 1,540 m/s, respectively. Speed errors result when the actual propagation speed through a tissue varies from the calibrated velocity used by the system (1,540 m/s). This leads to inaccurate measurements between tissue boundaries. As a result of slower propagation of sound through the fatty mass, the portion of the diaphragm-lung interface deep to the myelolipoma (yellow line) is incorrectly positioned further from the probe than the adjacent interface deep to the liver (white line). Although the diaphragm-lung interface is smooth and continuous in reality, it takes on an artifactual stair-stepped appearance on ultrasound.
|
4c What is the most likely diagnosis for this lesion?
A. Adrenal myelolipoma
B. Renal cell carcinoma
C. Adrenal cortical carcinoma
D. Adrenal hemorrhage
View Answer
4c Answer A. Although renal cell carcinomas may contain fat (from lipid-producing necrosis, intratumoral osseous metaplasia with fatty marrow elements, and entrapment of perirenal or sinus fat), we would not expect them to be composed primarily of fat. Renal angiomyolipomas, adrenal myelolipomas, and retroperitoneal liposarcoma can be mostly or purely composed of fat on imaging. There are case reports of adrenal cortical carcinoma containing macroscopic fat, but in virtually all cases, the presence of macroscopic fat within an adrenal mass permits a diagnosis of a benign lesion.
4d What is the likelihood of malignant transformation of adrenal myelolipomas?
A. 0%
B. 10%
C. 30%
D. 50%
View Answer
4d Answer A. There is no recognized malignant potential for adrenal myelolipomas.
References: Kenney PJ, Wagner BJ, Rao P, et al. Myelolipoma: CT and pathologic features. Radiology 1998;208(1):87-95.
Rumack CM, Wilson SR, Charboneau WJ. Diagnostic ultrasound, 4th ed. Philadelphia, PA: Elsevier Health Sciences, 2011:3-4.
5 The ultimate goal of root cause analysis (RCA) is to:
A. Identify individuals responsible for serious adverse events
B. Eliminate active errors
C. Eliminate latent errors
D. Identify the single root cause of an adverse event
View Answer
5 Answer C. Root cause analysis is a structured method borrowed from analysis of industrial accidents to evaluate serious adverse events. It is a comprehensive process requiring data collection, event reconstruction, record review, and interviews. Both active errors, those leading directly to the event, and latent errors, hidden errors within the health care system contributing to the error, are studied. This information is analyzed by a multidisciplinary team to determine how and why the event occurred. The ultimate goal of RCA is to eliminate the various latent errors, which contribute to an increased risk of similar future errors. Rather than a single root cause, often adverse events are caused by multiple errors and system flaws.
Reference: American Board of Radiology. Quality and Safety Domain Specification and Resource Guide, Core Exam Study Guide. Tucson, AZ: ABR, 2016:28.
6 According to the Joint Commission, “a sentinel event is an unexpected occurrence involving death or serious physical or psychological injury, or the risk thereof.” These events signal the need for immediate investigation and response. Which of the following sentinel events between 2004 and 2014 had the highest reported incidence?
A. Radiation overdose
B. Anesthesia-related event
C. Medication error
D. Wrong patient, wrong site, wrong procedure
View Answer
6 Answer D. Between 2004 and 2014, there were 1,072 reports of wrong-patient, wrong-site, wrong-procedure sentinel events, representing the largest category. Radiation overdoses, anesthesia-related events and medication errors accounted for 36, 104 and 428 events, respectively.
Reference: American Board of Radiology. Quality and Safety Domain Specification and Resource Guide, Core Exam Study Guide. Tucson, AZ: ABR, 2016:26.
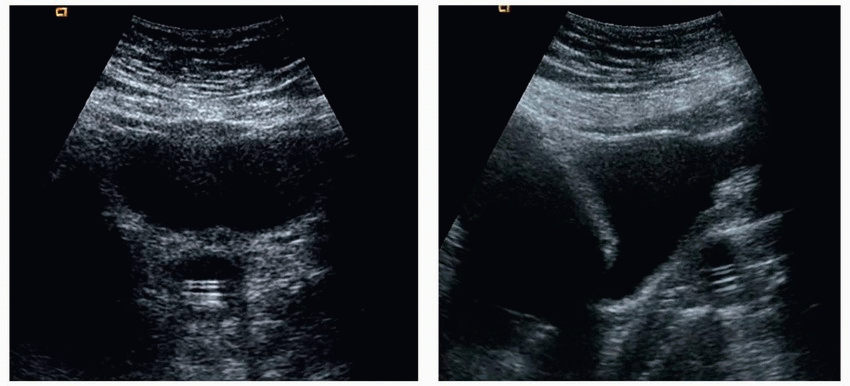
7a A 53-year-old female patient presents with low urine output. Transverse and sagittal US images of bladder are shown. What is the most likely diagnosis?
|
A. Bladder diverticulum
B. Ureterocele
C. Urachal cyst
D. Malpositioned Foley
E. Gartner cyst
View Answer
7a Answer D. Images show a Foley balloon posterior to the bladder with catheter extending caudally in the vagina.
Bladder diverticula typically occur in the setting of bladder outlet obstruction. Connection to the bladder is usually seen sonographically. Urethral diverticula arise from and are immediately associated with the urethra. They are best seen on ultrasound by transvaginal or transperineal imaging. Ureteroceles are formed from cystic dilatation of the intravesical segment of the ureter. On ultrasound, they appear as cystic structures in the posterolateral bladder (expected insertion of ureter). Urachal cysts occur because of incomplete closure of the urachus and are therefore located along the anterior and superior aspect of the bladder. Although Gartner duct cysts are located in this location (anterior lateral vagina above the pubic symphysis), the structure shown in this image is clearly a Foley catheter with balloon in the midline vagina and catheter segment extending through the balloon and caudally in the vagina.
7b What is the most common histology for a neoplasm arising within a urachal cyst?
A. Adenocarcinoma
B. Clear cell
C. Squamous cell
D. Transitional cell
7c Which key imaging feature of a Gartner duct cyst distinguishes it from other cystic lesions in the female pelvis?
A. Location in the anterolateral vagina above the pubic symphysis
B. Direct communication with the urethra
C. Location in the wall of the cervix
D. Location in the posterior lateral aspect of the inferior one-third of the vagina
View Answer
7c Answer A. Gartner duct cysts are typically located in the anterior lateral vaginal wall above the pubic symphysis. They may be seen in association with other wolffian anomalies such as renal agenesis and ectopic ureter. Urethral diverticula can be confused with Gartner duct cysts because of similar location and appearance. Urethral diverticula will show direct communication with the urethra. Bartholin duct cysts are located in the posterior lateral inferior third of the vagina below the level of the pubic symphysis. Nabothian cysts are located within the wall of the cervix.
References: Berrocal T, López-Pereira P, Arjonilla A, et al. Anomalies of the distal ureter, bladder, and urethra in children: embryologic, radiologic, and pathologic features. Radiographics 2002;22(5):1139-1164.
Chaudhari VV, Patel MK, Douek M, et al. MR imaging and US of female urethral and periurethral disease. Radiographics 2010;30(7):1857-1874.
Yu J-S, Kim KW, Lee H-J, et al. Urachal remnant diseases: spectrum of CT and US findings. Radiographics 2001;21(2):451-461.
8 Combining images from the same site using different scanning angles to reduce image speckle and improve delineation of tissue interfaces is termed:
A. Spatial compounding
B. Tissue harmonic imaging
C. Three-dimensional ultrasound
View Answer
8 Answer A. Spatial compounding combines images obtained from different scan angles into a single frame. By utilizing multiple scan angles, lesion margins are better delineated because more of the lesion margin is close to 90 degrees to the ultrasound beam. Orientation of a specular reflector 90 degrees to the beam maximizes the amount of reflected acoustic energy returning to the probe, leading to more distinct boundaries for cysts and other masses. Additionally, although desirable acoustic interfaces such as those found in renal cysts are reinforced through the summing of the images, randomly located speckle noise is not reinforced, resulting in a significantly increased signal-to-noise ratio.
Reference: Rumack CM, Wilson SR, Charboneau WJ. Diagnostic ultrasound, 4th ed. Philadelphia, PA: Elsevier Health Sciences, 2011:14-16.
9 What is the clinical significance of side-lobe artifacts?
A. They can produce the appearance of debris or tissue within fluid-filled structures.
B. They can create the false impression of a duplicated structure such as the abdominal aorta.
C. They can create a series of regularly spaced echoes at increasing depth.
D. They can result in impaired penetration of deeper structures.
View Answer
9 Answer A. Side lobes are located outside of the primary desired acoustic beam but may interact with tissues and return as an echo to the probe, thus creating artifactual low-level echoes, which are best appreciated within anechoic cystic and fluid-filled structures. For example, side-lobe artifact can result in the appearance of gallbladder sludge.
Reference: Rumack CM, Wilson SR, Charboneau WJ. Diagnostic ultrasound, 4th ed. Philadelphia, PA: Elsevier Health Sciences, 2011:17.
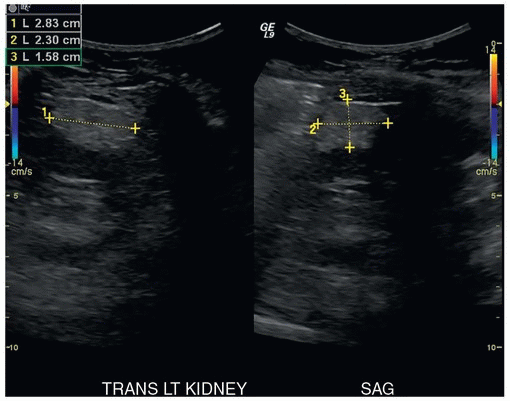
10a The patient here has a history of epilepsy and had an unwitnessed seizure. He is now complaining of left upper quadrant pain and presents to the emergency department where an abdominal ultrasound is ordered to evaluate the pain. The scan showed no free fluid, hematoma, or other findings suspicious for trauma, but the renal lesion shown was incidentally noted on the scan. Based on the history and imaging findings, what other extrarenal findings might this patient have?
|
A. Acanthosis nigricans
B. Cherry angiomas
C. Facial sebaceous adenomas
D. Clubbing of the nails
View Answer
10a Answer C. The images show a homogeneously echogenic lesion at the upper pole of the left kidney, with a maximal diameter of slightly <3 cm. The imaging features are characteristic of an angiomyolipoma. AMLs are benign tumors composed of dysmorphic vessels, smooth muscle, and mature fat. Eighty percent are sporadic, most frequently in middle-aged women, and the other 20% are associated with tuberous sclerosis (TS). Patients with TS often have mental retardation, seizures, and facial sebaceous adenomas. Therefore, C is the correct answer. None of the other choices are associated with TS.
10b Which of the following would be the most appropriate next step?
A. A course of antibiotics and follow-up with urology
B. CT scan to document the presence of fat
C. CT scan of the abdomen and pelvis to assess for lymphadenopathy
D. Consult with interventional radiology for embolization
View Answer
10b Answer B. Although a homogeneous, highly echogenic mass is very suggestive of AML, approximately 10% of renal cell carcinoma (RCC) can mimic this appearance. One distinguishing feature seen in up to 30% of AMLs is acoustic shadowing, which is extremely rare in RCC. Hyperechoic masses that show no acoustic shadowing require further characterization with CT or MRI to demonstrate fat. Choice B is the correct answer. Choice A is not correct because the lesion is neoplastic, not inflammatory. Choice C would not be the most appropriate next step because the lesion is statistically an AML, and confirmation of fat is likely all that is needed. Although bleeding is a serious complication related to AMLs, it is rare when the lesions are <4 cm. Therefore, choice D is incorrect.
Reference: Hertzberg BS, Middleton WD. Ultrasound: the requisites, 3rd ed. Philadelphia, PA: Elsevier, 2016:122-123.
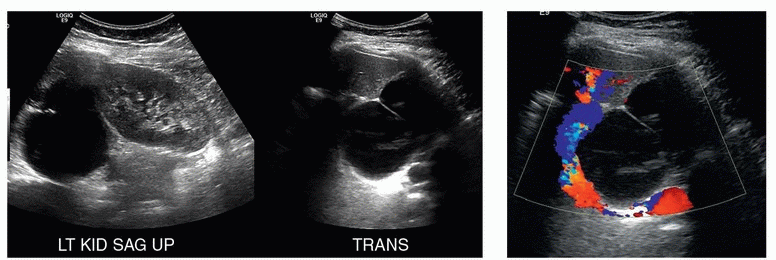
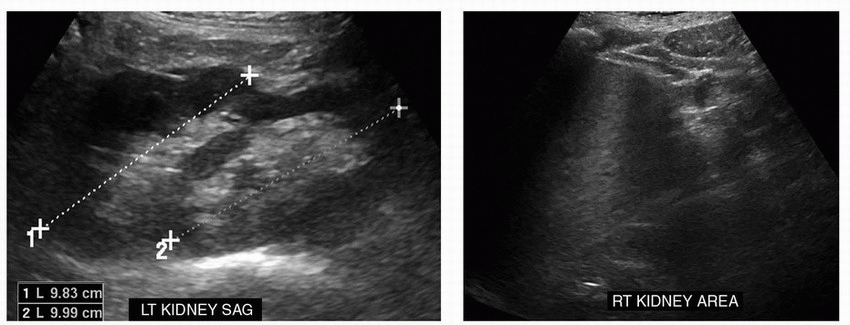
11a Two images are provided from a renal ultrasound on an asymptomatic patient. Which of the following is the best diagnosis?
|
A. Right pelvic kidney
B. Horseshoe kidney
C. Diffuse compensatory hypertrophy of the left kidney after right nephrectomy
D. Crossed fused renal ectopia
View Answer
11a Answer D. The images show an absent kidney in the right renal fossa. There are two normal-sized kidneys broadly fused together in the left renal fossa. At real time, the kidneys in this patient extended into the left lower pelvis. A pelvic right kidney (choice A) is incorrect because pelvic kidneys are not fused to the contralateral kidney. They remain on the ipsilateral side of the body but are found more inferiorly. Horseshoe kidneys are usually fused at the lower poles and located more inferiorly than normal, but each renal moiety will remain in the correct side of the body (option B). Diffuse compensatory hypertrophy results in ipsilateral renal enlargement when the contralateral kidney is absent or dysfunctional (option C), particularly when the renal insult occurs in utero or early in life. The right kidney in this case is present and normal appearing, but is abnormally positioned.
11b In crossed fused renal ectopia, the location of the ureterovesical junction of the ectopic kidney:
A. Is associated with a ureterocele
B. Inserts on the contralateral side of the bladder
C. Is normally located
D. Is prone to reflux
View Answer
11b Answer C. Crossed renal ectopia occurs when there is in utero fusion of the metanephrogenic blastema, not allowing for proper renal rotation or ascent. The ureterovesical junctions are not affected, and both are in normal anatomical location. This is useful to remember when these patients present with renal colic.
References: Hertzberg BS, Middleton WD. Ultrasound: the requisites, 3rd ed. Philadelphia, PA: Elsevier, 2016:103-106.
Rumack CM, Wilson SR, Charboneau WJ. Diagnostic ultrasound, 4th ed. Philadelphia, PA: Elsevier Health Sciences, 2011:324.
12 During review of a right upper quadrant ultrasound for pain, a radiologist makes a diagnosis of an acute cholecystitis. On a CT scan performed 1 year later, a right renal mass is discovered. In retrospect, this was definitely present on the ultrasound and had grown in the interval. This is an example of what category of radiologist error?
A. Perceptual error
B. Cognitive error
C. Negligence
D. Selection bias
View Answer
12 Answer A. The two broad categories of radiologist error are perceptual and cognitive (interpretive) errors. Perceptual error occurs when an abnormality that can be seen in retrospect was not identified by the interpreting radiologist at the time of the initial interpretation. “Satisfaction of search,” in which identification of one abnormality results in a second abnormality being overlooked, is one of many potential causes of perceptual error. Perceptual errors account for 60% to 80% of radiologists’ errors. Cognitive error occurs when the radiologist identifies a finding but renders an incorrect interpretation.
Reference: American Board of Radiology. Quality and Safety Domain Specification and Resource Guide, Core Exam Study Guide. Tucson, AZ: ABR, 2016:26.
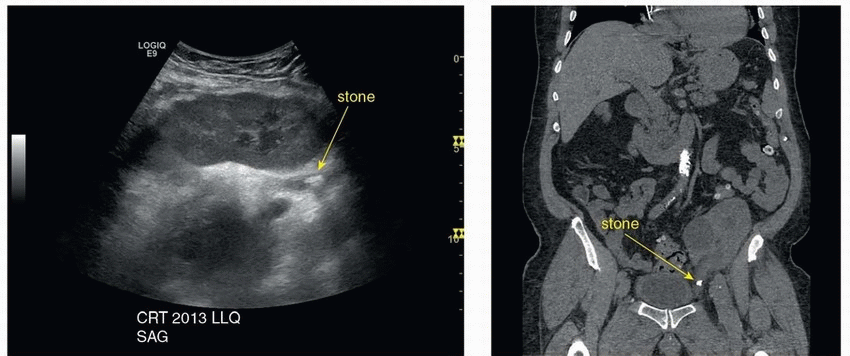
13 A patient with a kidney transplant was being evaluated for a new elevation of creatinine levels. Two sagittal color Doppler images at the hilum and a transverse image through the lower pole of the left pelvic kidney transplant were obtained. What is the most significant abnormality depicted on the image?
|
A. A perinephric fluid collection causing severe renal vein stenosis
B. An obstructing ureteral stone causing mild hydronephrosis
C. Subcapsular hematoma
D. Posttransplant lymphoproliferative disease
View Answer
13 Answer B. The ultrasound shows a shadowing stone that was glimpsed on the sagittal and transverse views in the proximal transplant ureter resulting in mild hydronephrosis. This is most likely the cause of the elevated creatinine level. The ultrasound images also reveal a simple-appearing deep perinephric collection near the renal vein. Although color Doppler aliasing and perhaps some luminal compression of the renal vein may be present, angle correction was not applied and a velocity gradient was not measured, so the provided images are not sufficient to diagnose severe renal vein stenosis (option A). The perinephric fluid collection shown remained stable 1 year later and was thought to represent a lymphocele. Subcapsular hematoma and solid masses, as can be seen with posttransplant lymphoproliferative disease, are absent (options C and D).
The clinical diagnosis of obstructive uropathy after renal transplant is difficult because the graft is denervated and patients are asymptomatic. The diagnosis may remain unsuspected until hydronephrosis or declining renal function is discovered incidentally. Mild, nonobstructive pelvicaliectasis is common after renal transplant.
|
References: Rhee BD, Bretan PN Jr, Stoller ML. Urolithiasis in renal and combined pancreas/renal transplant recipients. J Urol 2005;161(5):1458-1462.
Rumack CM, Wilson SR, Charboneau WJ. Diagnostic ultrasound, 4th ed. Philadelphia, PA: Elsevier Health Sciences, 2011:679-681.
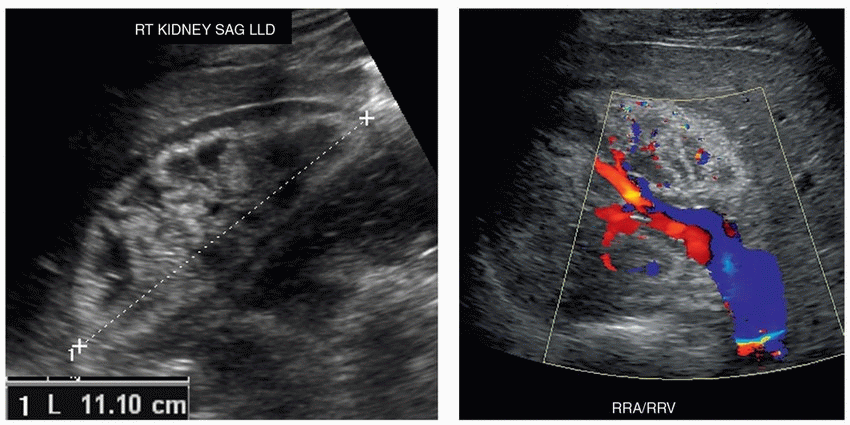
14 A 20-year-old male with proteinuria and azotemia undergoes a renal ultrasound to rule out hydronephrosis. Sagittal and transverse views of the right kidney are provided. Both kidneys had the same appearance. What is the most likely cause of this patient’s renal dysfunction?
|
A. Membranous glomerulonephritis
B. Renal vein thrombosis
C. Hydronephrosis
D. Xanthogranulomatous pyelonephritis
View Answer
14 Answer A. Sonography is often used as a screening tool in patients presenting with elevated creatinine to rule out underlying mechanical obstruction. Lack of obstruction usually indicates that renal parenchymal disease is present. Sonographic appearance of various renal parenchymal diseases such as acute tubular necrosis, glomerulonephritis, and acute interstitial nephritis affecting the kidneys is difficult to distinguish on ultrasound. Patients often present with diffusely echogenic kidneys, and biopsy may be needed in select patients to establish a specific diagnosis. The images show a mildly enlarged, strikingly echogenic cortex relative to the spleen (when the spleen is used as an external control) and the hypoechoic renal pyramids (when used as an internal control).
The color Doppler image of the renal vein confirms patency, and there is no dilatation of the renal pelvis (choices B and C are incorrect). The hypoechoic rim around the kidney represents perinephric fat, which appears hypoechoic relative to the echogenic renal cortex. Diffuse xanthogranulomatous pyelonephritis does not have specific sonographic features but can be suggested when renal enlargement, cortical thinning, dilated, debris-filled calyces, large calculi, and perinephric fluid are present (option D). This particular patient had a known history of idiopathic membranous glomerulonephritis, an autoimmune disease.
References: Hertzberg BS, Middleton WD. Ultrasound: the requisites, 3rd ed. Philadelphia, PA: Elsevier, 2016:131-132.
Makker SP, Tramontano A. Idiopathic membranous nephropathy: an autoimmune disease. Semin Nephrol 2011;31(4):333-340.
Rumack CM, Wilson SR, Charboneau WJ. Diagnostic ultrasound, 4th ed. Philadelphia, PA: Elsevier Health Sciences, 2011:380-382.
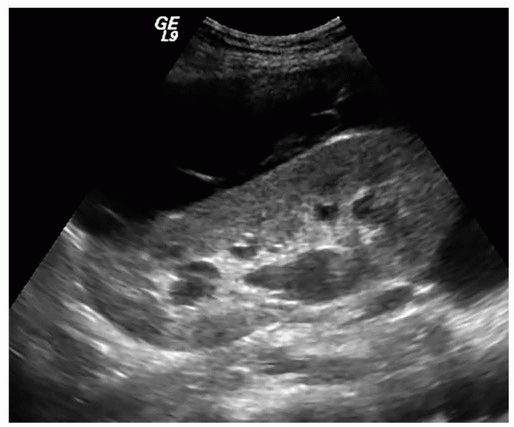
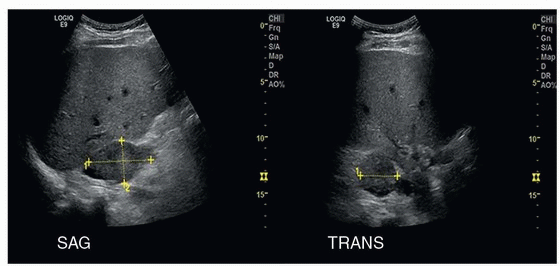
15 A 36-year-old male presents with left lower quadrant pain 3 weeks following renal transplant. Sagittal ultrasound image of the left lower quadrant renal allograft is provided. What is the most likely diagnosis?
|
A. Urinoma
B. Lymphocele
C. Hematoma
D. Abscess
View Answer
15 Answer B. Sagittal ultrasound image of the left lower quadrant renal allograft shows a large anechoic peritransplant fluid collection with few internal septations. This most likely represents a peritransplant lymphocele. Lymphoceles are the most common fluid collections seen in renal transplant recipients. They typically occur 1 to 3 weeks following surgery. They may be asymptomatic or cause local pain and tenderness. Septations may be seen within lymphoceles, as in this case. Lymphoceles form from leakage of lymph from recipient lymphatic channels. Large lymphoceles may result in impaired graft function.
Urinomas are much less common. They occur because of breakdown of the ureter implantation into the bladder. Therefore, they are usually in close proximity to and may exert mass effect on the bladder. Hematomas are common in the early postoperative period. Small hematomas may be seen incidentally at imaging. Large hematomas may result in pain. At ultrasound, hematomas usually appear as heterogeneous perinephric collections. Abscesses typically appear as complex fluid collections containing internal debris.
References: Hertzberg BS, Middleton WD. Ultrasound: the requisites, 3rd ed. Philadelphia, PA: Elsevier, 2016:140-141.
Moreno CC, Mittal PK, Ghonge NP, et al. Imaging complications of renal transplantation. Radiol Clin North Am 2016;54(2):235-249.
16a A 42-year-old female with history of lung cancer presents with pelvic pain. Which of the following is the most likely diagnosis?
|
A. Nabothian cyst
B. Gartner duct cyst
C. Urethral diverticulum
D. Metastasis
E. Bartholin cyst
View Answer
16a Answer B. The images show an ovoid circumscribed cystic lesion containing low-level internal echoes within the wall of the upper vagina. There is posterior acoustic enhancement and no internal vascularity. The transvaginal probe indents the mass.
The wolffian (mesonephric) ducts, embryologic precursors to the vas deferens and seminal vesicles, regress in the absence of testosterone and antimüllerian hormone. Gartner duct cysts (GDCs) are rare remnants of regressed wolffian ducts. They are usually small (<2 cm) and located within the anterolateral aspect of the upper vagina.
 CT images with reformats demonstrate the Gartner duct cyst (arrow). |
Nabothian cysts are located within the cervix, not the vaginal wall. A urethral diverticulum is located around the urethra and not within the vaginal wall. It typically has a horseshoe shape. A metastasis should have some internal vascularity. A necrotic metastasis could have a complicated cystic appearance but would also have a more irregular wall. Careful scanning should show vascularity in solid mural components. Bartholin cysts are located at or below the level of the pubic symphysis and usually arise from the posterior vaginal wall.
16b Which of the following often requires surgery?
A. Nabothian cyst
B. Gartner duct cyst
C. Ureterocele
D. Müllerian cyst
E. Bartholin cyst
View Answer
16b Answer C. Nabothian cysts, GDCs, müllerian cysts, and Bartholin cysts are usually incidental findings.
Ureteroceles may require surgical repair. Asymptomatic orthotopic ureteroceles can be incidental. Symptomatic orthotopic ureteroceles may require repair, though this can usually be done endoscopically. Most ectopic ureteroceles require intervention. Those inserting on the bladder may be repaired endoscopically; those inserting outside the bladder usually require open repair. In the congenitally duplicated urinary tract, the obstructing ectopic ureterocele of the upper pole moiety usually also requires open surgery.
References: Lui M-W, Ngu S-F, Cheung VYT. Mullerian cyst of the uterus misdiagnosed as ovarian cyst on pelvic sonography. J Clin Ultrasound 2013;42(3):183-184.
Siegelman ES. Body MRI. Philadelphia, PA: Elsevier Health Sciences, 2005:291-292, 329-330, 418.
17a Which of the following choices represents the most appropriate next step in workup of this incidental sonographic finding?
|
A. Follow-up ultrasound in 6 months
B. Surgical excision
C. CT or MRI
D. Biopsy
View Answer
17a Answer C. Images show a sharply demarcated partially exophytic solid-appearing left lower pole renal mass isoechoic to the renal parenchyma, which contains a few punctate calcifications. The differential diagnosis for a solid renal mass includes renal cell carcinoma (RCC), angiomyolipoma, oncocytoma, transitional cell carcinoma, lymphoma, and metastasis.
Transitional cell carcinoma and lymphoma typically have a more infiltrative appearance and do not typically result in discrete exophytic masses. Additionally, the cortical epicenter of this mass argues against a urothelial origin. Angiomyolipomas are typically hyperechoic and rarely contain calcification. Renal oncocytomas are usually impossible to distinguish from RCCs preoperatively but rarely contain calcification. Metastasis can be considered if there is a known malignancy.
Although this mass should be presumed to represent a renal cell carcinoma based on its solid appearance, a CT or MRI would be an important study to perform prior to surgery for staging. Renal mass biopsy is usually limited to cases in which the diagnosis of lymphoma or metastasis is suspected, as these are not treated with surgical resection, or to cases in which the patient is not a surgical candidate.
17b In the absence of detectable Doppler flow within this mass, what is the most appropriate management of this finding?
A. Follow-up ultrasound in 6 months
B. Surgical excision
C. CT or MRI
D. Biopsy
View Answer
17b Answer C. Although the presence of intralesional Doppler flow indicates a solid renal mass and a renal cell carcinoma with a high degree of certainty, the absence of detectable flow does not exclude a neoplasm. One reason is that some renal cell carcinomas are hypovascular, although highly vascular tumors will also usually exhibit less Doppler signal than the surrounding renal parenchyma. The sensitivity for detection of flow is also decreased when interrogating deeper lesions. In the setting of an indeterminate renal mass, CT or MRI is necessary for lesion characterization and detection of enhancement. Contrast-enhanced ultrasound is also emerging as a highly sensitive method for identifying blood flow within tumors.
|
References: Dyer R, DiSantis DJ, McClennan BL. Simplified imaging approach for evaluation of the solid renal mass in adults. Radiology 2008;247(2):331-343.
Hertzberg BS, Middleton WD. Ultrasound: the requisites, 3rd ed. Philadelphia, PA: Elsevier, 2016:114-120.
Siegel CL, Middleton WD, Teefey SA, et al. Angiomyolipoma and renal cell carcinoma: US differentiation. Radiology 1996;198(3):789-793.
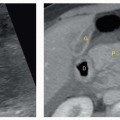
18a An ultrasound of the urinary bladder was performed for a patient with recurrent urinary tract infections. Selected images of the midline tissues superior to the bladder are shown. What is the most likely diagnosis?
|
A. Adhesion
B. Appendicitis
C. Urachal diverticulum
D. Ectopic ureter
View Answer
18a Answer C. Deep to the anterior abdominal wall, a tubular blind-ending structure extends superiorly from the bladder dome. It contains a small amount of fluid. Close inspection reveals a mucosal lining throughout the structure. Findings are compatible with a urachal diverticulum. See additional CT images with multiplanar reformats on the next page. Arrows denote the diverticulum.
The urachus is the fibrous vestige of the fetal allantois, a tubular structure through which urine drains from the bladder dome to the umbilicus during the first trimester of pregnancy. Normally, this channel obliterates after the first trimester of pregnancy, leaving the median umbilical ligament, located within the extraperitoneal space of Retzius.
Incomplete obliteration results in a spectrum of urachal disorders. A patent urachus allows urine to leak from the bladder to the umbilicus. A urachal cyst is located along the urachus without communication to the umbilicus or bladder. A urachal sinus is a blind ending tract communicating with the umbilicus. A urachal diverticulum is a blind ending tract extending from the bladder.
|
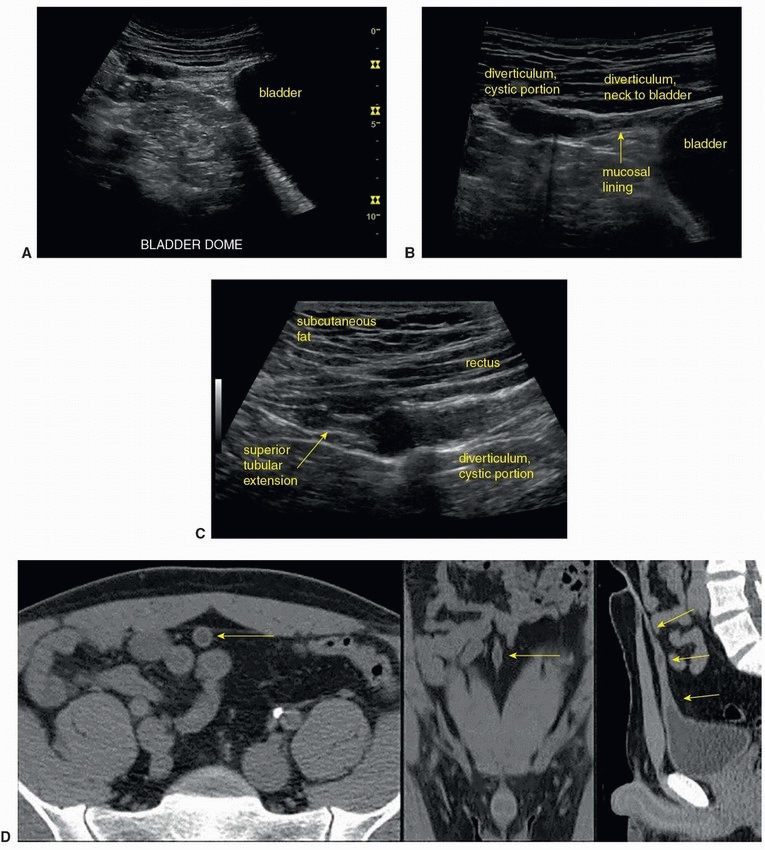
18b Which of the following is the most likely cause of a midline partially calcified soft tissue mass found behind the rectus sheath located between the umbilicus and bladder dome?
A. Umbilical hernia
B. Adenocarcinoma
C. Transitional cell carcinoma
D. Lymphoma
View Answer
18b Answer B. Urachal adenocarcinomas are a rare complication of urachal remnants. They may be located anywhere along the course of the urachus, including the bladder dome, and often have a large extravesical component. They are often large at presentation and often appear as partially calcified mixed solid and cystic masses.
References: Aguirre DA, Santosa AC, Casola G, et al. Abdominal wall hernias: imaging features, complications, and diagnostic pitfalls at multi-detector row CT. Radiographics 2005;25(6):1501-1520.
Gleason JM, Bowlin PR, Bagli DJ, et al. A comprehensive review of pediatric urachal anomalies and predictive analysis for adult urachal adenocarcinoma. J Urol 2015;193(2):632-636.
Yu J-S, Kim KW, Lee H-J, et al. Urachal remnant diseases: spectrum of CT and US findings. Radiographics 2001;21(2):451-461.
19 A 65-year-old man is found to have a well-defined homogeneous renal lesion on a contrast-enhanced CT measuring 50 HU and undergoes an ultrasound for further evaluation. Based on this image, which of the following choices best describes the lesion?
|
A. Simple cyst
B. Complicated cyst
C. Cystic renal cell carcinoma
D. Indeterminate
View Answer
19 Answer D. Renal lesions, which are higher in attenuation than water but well-defined and homogeneous, are usually best evaluated with a sonogram, as most of these lesions represent benign cysts and can be effectively confirmed to be anechoic simple cysts on ultrasound. In this example, the lesion margins are indistinct, an unexpected finding given its sharply circumscribed appearance on CT. The renal capsule is also indistinct in spite of its fairly superficial location. These findings indicate that the lesion is not optimally visualized and should trigger a review of the technical parameters and scan technique. Settings for both depth of field and focal zone are too deep and should be corrected. Depth of field much greater than the lesion depth decreases axial spatial resolution. Because the focal zone is much deeper than the lesion, lateral resolution is also compromised. Once these parameters are corrected, the probe transmit frequency can also be maximized to further improve image quality.
Optimized image of the left kidney is shown. The lesion represents a simple benign renal cyst.
|
Reference: Hertzberg BS, Middleton WD. Ultrasound: the requisites, 3rd ed. Philadelphia, PA: Elsevier, 2016:109-111.
20 A 65-year-old patient presents with chronically elevated creatinine and new oliguria. Which of the following is the most likely diagnosis?
|
A. Xanthogranulomatous pyelonephritis
B. Emphysematous pyelitis
C. Renal abscess
D. Emphysematous pyelonephritis
View Answer
20 Answer B. There is mild hydronephrosis, and multiple linear high-amplitude echoes with posterior dirty acoustic shadowing representing gas are located within the renal pelvis. Findings are compatible with emphysematous pyelitis, a urinary tract infection characterized by the presence of gas within the collecting system. This diagnosis can be made once other causes of gas including recent instrumentation, trauma, and fistulous communication with bowel are excluded. Emphysematous pyelitis usually responds to antibiotic therapy without the need for an invasive procedure. It is important to perform a CT in order to confirm the absence of renal parenchymal gas.
 Coronal reformat from the patient’s CT scan shows presence of gas in the collecting system. |
Emphysematous pyelonephritis (EPN) is a severe life-threatening necrotizing renal parenchymal infection usually occurring in patients with uncontrolled diabetes. It is characterized by the presence of renal parenchymal gas. Xanthogranulomatous pyelonephritis (XGP) is a rare chronic granulomatous pyelonephritis resulting in a nonfunctioning kidney. Various bacteria implicated with XGP include Escherichia coli and Proteus mirabilis. In 90% of cases, a staghorn calculus with hydronephrosis is present. The kidney is eventually replaced by an inflammatory mass, composed predominantly of lipid-laden macrophages. The inflammatory process may involve the perinephric tissues or even nearby organs. The sonographic diagnosis can be challenging because of a lack of specific imaging findings, but the possibility of XGP should be considered if parenchymal thinning, hydronephrosis with stones and debris, and perinephric fluid collections are present. In this example, gas and collecting system dilatation are the only abnormalities.
Renal abscess usually appears as a complex fluid collection or complex cystic masses. In the case shown here, the high-amplitude echoes representing gas are clearly within the renal pelvis and not within a separate fluid collection or cystic mass.
References: Craig WD, Wagner BJ, Travis MD. Pyelonephritis: radiologic-pathologic review. Radiographics 2008;28(1):255-276.
Hertzberg BS, Middleton WD. Ultrasound: the requisites, 3rd ed. Philadelphia, PA: Elsevier, 2016:124-125.
Rumack CM, Wilson SR, Charboneau WJ. Diagnostic ultrasound, 4th ed. Philadelphia, PA: Elsevier Health Sciences, 2011:336.
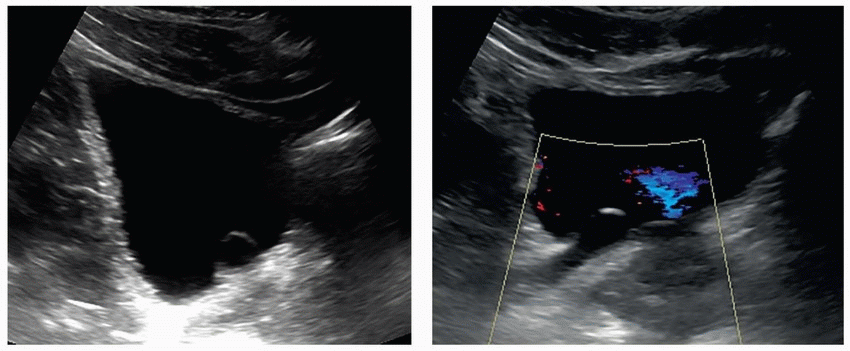
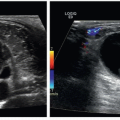
21 Based on the images, which of the following is a likely predisposing risk factor for the entity seen in these images in this otherwise healthy young male?
|
A. Nephrotic syndrome
B. Renal cell carcinoma
C. Smoking history
D. Crossed fused renal ectopia
View Answer
21 Answer A. Echogenic material within the right renal vein with adjacent color Doppler signal represents subocclusive thrombus. Spontaneous renal vein thrombosis is most commonly associated with malignancy, especially renal cell carcinoma, and nephrotic syndrome. Other causes include trauma, biopsy, oral contraceptives, hypovolemia, and inherited hypercoagulable states. Although renal vein thrombus in the setting of renal cell carcinoma usually represents tumor thrombus, the pathogenesis of renal vein thrombosis in the setting of nephrotic syndrome is poorly understood.
 Arrow denotes the subocclusive thrombus in the right renal vein. |
Reference: Hertzberg BS, Middleton WD. Ultrasound: the requisites, 3rd ed. Philadelphia, PA: Elsevier, 2016:138.
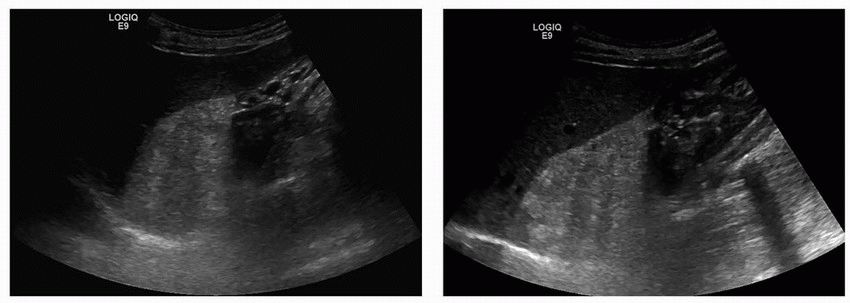
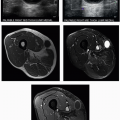
22 Images from right upper quadrant ultrasound of a 52-year-old male with history of non-small cell carcinoma of lung are shown. What is the next best step in the management of this patient?
|
A. The hyperechoic areas in the mass suggest myelolipoma. No further evaluation is needed.
B. The lesion is solid and almost certainly represents a perinephric metastasis. Confirm with percutaneous biopsy.
C. Minimal heterogeneity of the mass favors adrenal adenoma. Recommend follow-up imaging in 1 year to ensure stability.
D. Large size and heterogeneity favor metastasis, but it should be evaluated by adrenal mass protocol CT or MRI to exclude an adenoma prior to percutaneous biopsy.
View Answer
22 Answer D. Large size and heterogeneity favor metastasis, but it should be evaluated by adrenal mass protocol CT or MRI to exclude an adenoma prior to percutaneous biopsy.
Adrenal gland is the fourth most common site of metastasis, with lung, breast, melanoma, and lymphoma being the most common primary neoplasms. The masses are solid on sonography and may demonstrate internal heterogeneity. They are often indistinguishable from adenomas though they usually tend to be larger and heterogeneous.
This mass is predominantly hypoechoic, which is not a characteristic sonographic appearance for myelolipoma.
Although the lesion is solid and suspicious for metastasis, an adrenal adenoma cannot be excluded on ultrasound, and further evaluation must be performed with adrenal mass protocol CT or MRI before proceeding to an invasive procedure such as percutaneous biopsy.
Large size of the lesion and the heterogeneity favor metastasis over an adenoma. However, an atypical adenoma cannot be excluded, and hence, further evaluation must be performed with adrenal mass protocol CT or MRI before proceeding to percutaneous biopsy.
References: Hertzberg BS, Middleton WD. Ultrasound: the requisites, 3rd ed. Philadelphia, PA: Elsevier, 2016:221-226.
Rumack CM, Wilson SR, Charboneau WJ. Diagnostic ultrasound, 4th ed. Philadelphia, PA: Elsevier Health Sciences, 2011:430-441.
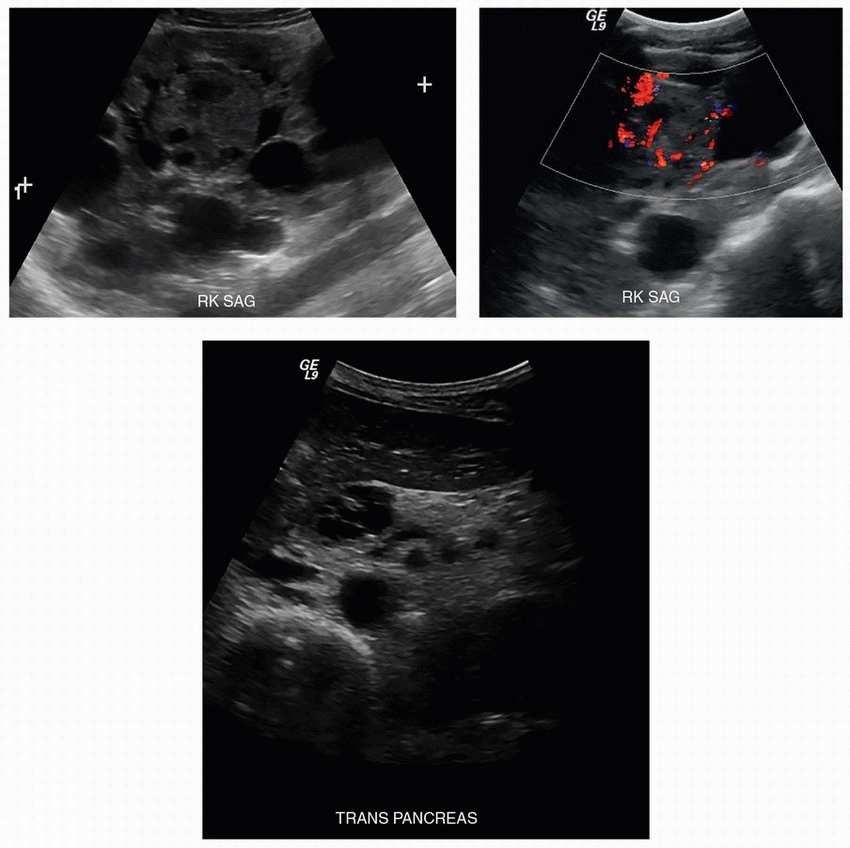
23a A 38-year-old male presents with hematuria. A renal ultrasound was performed. Sagittal images of the right kidney are provided. An incidental finding was noted in the pancreas as well. The patient’s sibling was diagnosed with the same condition 2 years prior. What is the most likely diagnosis?
|
A. Tuberous sclerosis
B. von Hippel-Lindau disease
C. Multiple endocrine neoplasia (MEN) I
D. Osler-Weber-Rendu syndrome
View Answer
23a Answer B. Gray-scale and color Doppler images of the right kidney show multiple renal cysts and a solid renal mass with internal vascularity. Transverse image through the head of the pancreas shows a pancreatic head cyst with septations. These imaging findings along with the indication of a family history suggest the diagnosis of von Hippel-Lindau disease (VHL). VHL disease is inherited in an autosomal-dominant fashion. Abdominal manifestations of VHL include simple pancreatic cysts, serous cystadenomas, pancreatic neuroendocrine tumors, benign renal cysts, renal clear cell carcinomas, and pheochromocytomas. Central nervous system manifestations include hemangioblastomas and retinal angiomas.
Tuberous sclerosis (TS) is an autosomal-dominant, neurocutaneous disorder. The common manifestations of TS include cortical or subependymal tubers and white matter abnormalities, angiomyolipomas, cardiac rhabdomyomas, lymphangioleiomyomatosis. Cutaneous manifestations are quite common and include facial angiofibromas (also called adenoma sebaceum), hypopigmented macules (ash-leaf spots), and ungual fibromas.
Multiple endocrine neoplasia type 1 (MEN1) is also inherited as an autosomal-dominant disorder. Manifestations include parathyroid, pancreatic, and pituitary tumors. Osler-Weber-Rendu syndrome also known as hereditary hemorrhagic telangiectasia (HHT) is an autosomal-dominant disorder that leads to the formation of dysplastic blood vessels in the skin and mucous membranes and in organs such as the lungs, liver, and brain.
23b Which additional imaging study should be performed and why?
A. MR brain to evaluate for subependymal tubers
B. Cardiac CT to evaluate for rhabdomyomas
C. MR brain to evaluate for intracranial AVMs
D. MR brain and spine to evaluate for hemangioblastomas
View Answer
23b Answer D. As stated above, central nervous system manifestations such as hemangioblastomas can be seen in patients with VHL. Therefore, D is the correct answer.
Subependymal tubers and cardiac rhabdomyomas are findings seen in tuberous sclerosis. Intracranial AVMs have no association with VHL disease. They can be seen in other rare phakomatoses such as Wyburn-Mason syndrome and Osler-Weber-Rendu syndrome.
Reference: Hertzberg BS, Middleton WD. Ultrasound: the requisites, 3rd ed. Philadelphia, PA: Elsevier, 2016:113-114.
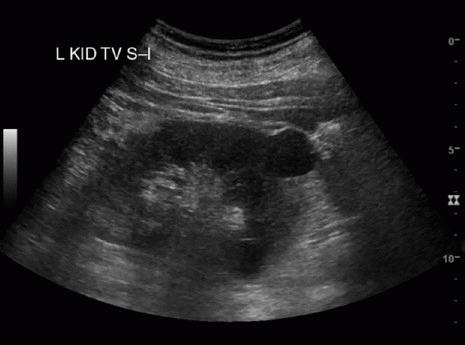
24a A 50-year-old female with long-standing history of affective disorder presents with renal failure. Sagittal image of the left kidney shows which of the following?
|

A. Renal microcysts
B. Renal cortical necrosis
C. Medullary nephrocalcinosis
D. Normal kidneys
View Answer
24a Answer A. Ultrasound image of the kidney shows multiple punctate echogenic foci located in both the renal medulla and cortex. The appearance is attributed to microcysts (1 to 2 mm) with fibrotic margins and possible internal calcification, which can be seen in patients treated long-term with lithium for affective disorders. This is a case of lithium nephropathy.
In renal cortical necrosis, one may see loss of normal corticomedullary differentiation and areas of increased echogenicity within the parenchyma. In medullary nephrocalcinosis, there is increased echogenicity of the renal pyramids due to calcium deposition.
24b Which of the following imaging tests may be used to confirm this finding?
A. CT scan
B. MRI
C. Renal scintigraphy
D. Plain radiograph
View Answer
24b Answer B. MR imaging has been demonstrated to be superior to ultrasonography and computed tomography for the visualization of small renal cysts. On MRI, small T2-hyperintense 1- to 2-mm round lesions are usually seen distributed randomly in the renal medulla and cortex.
Radionuclide techniques can demonstrate poor radiopharmaceutical excretion in diffuse renal diseases. However, they are not disease specific. Plain radiographs will not be able to demonstrate the morphologic changes seen in the kidneys in lithium nephropathy.
References: Di Salvo DN, Park J, Laing FC. Lithium nephropathy. J Ultrasound Med 2012;31(4):637-644.
Farres MT, Ronco P, Saadoun D, et al. Chronic lithium nephropathy: MR imaging for diagnosis. Radiology 2003;229(2):570-574.
25 A 47-year-old male with right flank pain undergoes an ultrasound. Images of the bladder are shown. What is the best diagnosis based on these findings?
|
A. Ureterocele
B. Bladder diverticulum
C. Hematoma or fungal ball
D. Pseudoureterocele
View Answer
25 Answer A. The thin-walled cystic bulbous structure located at the right ureterovesical junction projecting into the bladder lumen represents a simple ureterocele. Dilatation of the ureterocele and upstream ureter and absence of a right ureteral jet on this image does not necessarily imply obstruction. Ureteroceles can be observed to grow and shrink in real time as they fill and empty with urine. A ureteral jet will also be visible as they empty. Ureteroceles are congenital focal dilatations of the intramural portion of the distal ureters. They are classified as simple, occurring at the normal ureteral orifice, or ectopic, occurring at another site such as the bladder neck, urethra, or vagina. In adults, most ureteroceles are simple. Small ureteroceles are usually incidental and not the cause of the patients’ symptoms, but larger ureteroceles >2 cm are more likely to result in obstruction or contain calculi. In children, ectopic ureteroceles are more common and are associated with complete ureteral duplication with ureteral obstruction.
Pseudoureteroceles are acquired dilatations of the ureterovesicle junction as a result of obstruction of the ureteral orifice. These can arise from stones, tumors, or recent manipulation. They can be recognized by the presence of an obstructing lesion or wall thickening.
References: Hertzberg BS, Middleton WD. Ultrasound: the requisites, 3rd ed. Philadelphia, PA: Elsevier, 2016:170.
Zagoria RJ, Dyer R, Brady C. Genitourinary imaging: the requisites, 3rd ed. Philadelphia, PA: Elsevier, 2016:153-156.
26 A 47-year-old male presents with hematuria. Images from abdominal ultrasound are shown. The patient is at increased risk for which of the following?
|
A. Renal cell carcinoma
B. Hypertension
C. Portal hypertension
D. Renal atrophy
View Answer




26 Answer B. The first two images show bilateral enlarged kidneys with innumerable renal cysts of varying sizes. The third image shows multiple hepatic cysts. This imaging appearance is consistent with autosomal-dominant polycystic kidney disease (ADPKD).
ADPKD is the most common hereditary renal cystic disease. The cysts are distributed diffusely throughout both kidneys and involve all portions of the kidneys. Extrarenal manifestations most commonly include hepatic cysts. Less commonly, pancreatic cysts, ovarian cysts, splenic cysts, arachnoid cysts, intracranial berry aneurysms with associated intracranial hemorrhage, abdominal aortic aneurysm, cardiac valve abnormalities, abdominal wall hernias, and colonic diverticula can be seen.
Renal complications of ADPKD include cyst hemorrhage, cyst infection, cyst rupture, and nephrolithiasis. About 50% of individuals with ADPKD develop end-stage renal disease. Intrarenal ischemia caused by continued renal cyst expansion with resultant activation of the renin-angiotensin-aldosterone system leads to hypertension. Therefore, choice B is the correct answer. The patient may present with flank and back pain, hypertension, or nephrolithiasis with eventual progression to renal failure.
There is no increased risk for renal cell carcinoma unless the patient is undergoing prolonged dialysis (choice A).
Portal hypertension (choice C) is not a feature of ADPKD. It is seen in autosomal recessive polycystic kidney disease (ARPKD). ARPKD is a heritable disorder characterized by nonobstructive renal collecting duct ectasia, hepatic biliary duct ectasia and malformation, and fibrosis of both liver and kidneys. In the kidney, the dilated collecting ducts and interstitial fibrosis may impair renal function and result in hypertension and renal failure. In the liver, periportal fibrosis accompanies the malformed and dilated bile ducts and may result in portal hypertension.
As mentioned earlier, the kidneys are enlarged bilaterally with multiple cysts present in ADPKD. Therefore, renal atrophy (choice D) is incorrect.
Related posts:



Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
