and Filiz Özülker1
(1)
Nuclear Medicine, Okmeydani Training and Research Hospital, Istanbul, Turkey
15.1 Case 1: Diagnosis of Renal Cell Carcinoma
History
A 51-year-old female is currently being evaluated for an incidentally detected right kidney mass. Patient underwent 18F-FDG PET/CT imaging before undergoing an operation.
Findings
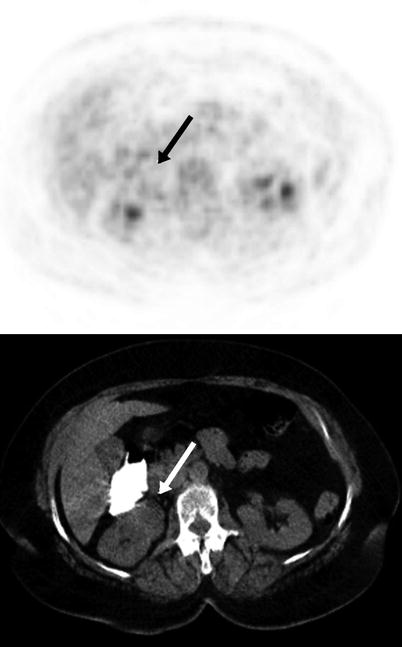
Fig. 15.1
Axial PET and CT images showed an anteromedially located cortical mass lesion with 2 cm diameter at right kidney (arrow). The lesion showed mild FDG uptake with a SUVmax of 2, which is not higher than renal parenchyma
Interpretation
Low level of FDG uptake at the lesion was suggestive of a benign lesion.
Result
Histopathological evaluation after operation revealed renal cell carcinoma (RCC).
Teaching Point
PET should have limited role in the characterization of primary renal tumors with its low sensitivity found as 62 % in a metaanalysis.
15.2 Case 2: False Positive Finding: Oncocytoma
History
A 59-year-old female is currently being evaluated for a mass lesion at left kidney detected on USG. The patient was scheduled for operation and meanwhile she underwent 18F-FDG PET/CT imaging.
Findings
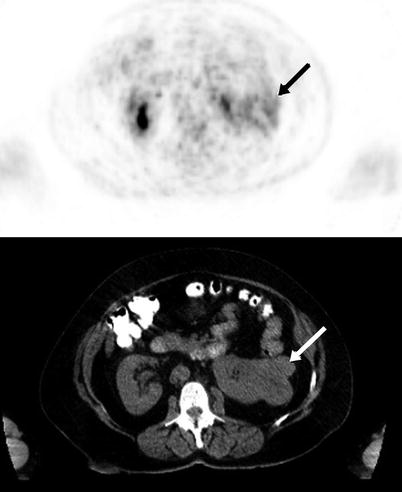
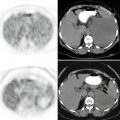
Fig. 15.2
Axial PET and CT images showed a lobulated mass lesion with 6.5 cm diameter, located at lateral cortex of left kidney (arrow). The lesion showed moderate FDG uptake with a SUVmax of 6.5
Interpretation
The lesion was suspicious for malignancy with its moderate FDG uptake.
Result
After operation the lesion turned out to be an oncocytoma.
Teaching Point
The pooled specificity of 18F-FDG PET/CT is found to be 88 % in the determination of malignant nature of kidney masses in a metaanalysis. Besides oncocytoma, there are several other benign lesions causing false positive FDG uptake like renal angiomyolipoma, renal pericytoma, nephroblastoma, renal tuberculosis, and xanthogranulomatous nephritis.
15.3 Case 3: Renal Cell Carcinoma Invading the Renal Vein
History
A 52-year-old female with a mass lesion originating from left kidney underwent 18 F-FDG PET/CT imaging.
Findings
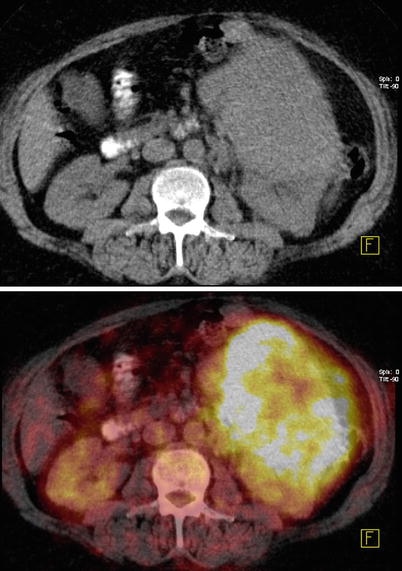
Fig. 15.3
Axial CT and fusion images showed a mass lesion with the dimensions of 11 × 12 × 14 cm originating from anterior cortex of left kidney (SUVmax 13.7)
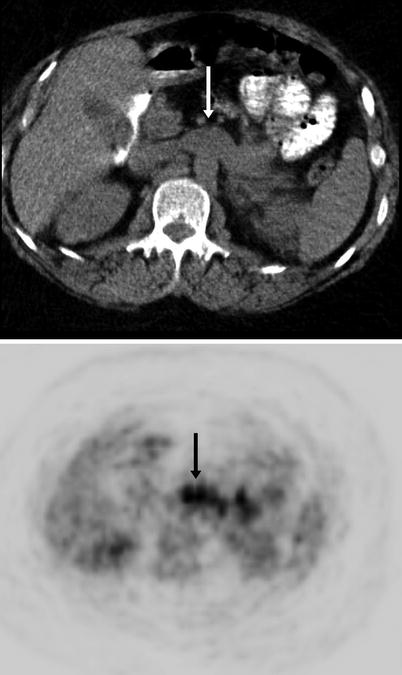
Fig. 15.4
Axial CT and PET images showing pathologically increased FDG uptake at left renal vein (arrow)

Fig. 15.5
MIP image showing intensely hypermetabolic left renal mass (black arrow), pathologically increased FDG uptake at left renal vein (white arrow)
Interpretation
Malignant lesion originating from left kidney and showing invasion to left renal vein.
Result
The patient underwent operation and histopathology revealed RCC invading left renal vein.
Teaching Point
18F-FDG PET/CT localizes RCC more efficiently in larger masses. One study showed an increase in sensitivity of FDG PET/CT from 76 to 92.9 % when the lesion size increased from more than 1–2 cm. RCC has a propensity to invade the venous system, with extension into the renal vein.
15.4 Case 4: Renal Cell Carcinoma Invading the Inferior Vena Cava and Right Atrium
History
A 52-year-old female suffering from weakness, weight loss, right-sided flank pain, and hematuria for 2 months. When she consulted with these symptoms, tenderness in the right flank region and hepatomegaly was detected on physical examination. The patient underwent CT scan with iv contrast, and besides the mass lesion at right kidney, a filling defect in IVC extending to the right atrium, which was strongly suggestive of tumor thrombus was detected. 18F-FDG-PET/CT scan was performed in order to make metabolic characterization of the right renal mass together with the thrombus in IVC.
Findings
Fig. 15.6
Axial CT and fusion images show pathologically increased FDG uptake at right atrium (arrow) (a, b) and the thrombus at IVC (arrow) (c, d)
Fig. 15.7
Coronal CT and PET images of 18F-FDG-PET/CT study showed intense FDG uptake in tumor thrombus in IVC (arrows) extending into right atrium and moderate FDG uptake in circular fashion in the right renal mass (a, b); sagittal CT and PET images show intense FDG uptake at thrombus in IVC (arrows) (c, d)
Interpretation
FDG avid malignant lesion originating from right kidney and intensely hypermetabolic tumor thrombus in IVC extending into right atrium.
Result
The patient underwent right nephrectomy and biopsy was obtained from tumor thrombus in the IVC. The histopathology of the mass from the right kidney and thrombus in the IVC revealed RCC.
Teaching Point
RCC has a propensity to invade IVC occurring in 4–10 % of all patients with RCC. Among these patients, 2–16 % have tumors extending into the right atrium.
15.5 Case 5: Renal Cell Carcinoma Metastasis to Maxillary Sinus
History
A 52-year-old male who has a history of renal cell carcinoma status post left nephrectomy and chemotherapy suffered from intermittent episodes of epistaxis and sinusitis. The patient underwent nasal endoscopy that diagnosed a tumor in the left maxillary sinus and biopsy was performed. Further evaluation with 18F-FDG PET/CT imaging was done to determine the extent of metastatic disease.
Findings
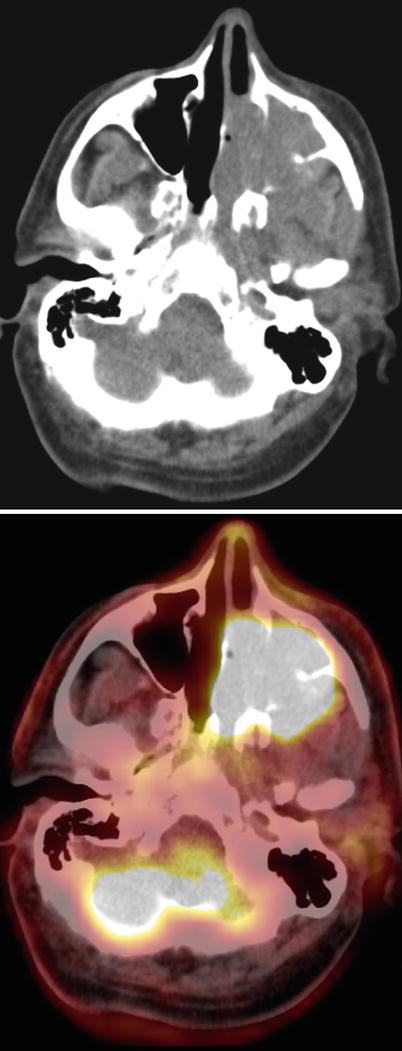
Fig. 15.8
Axial CT and fusion images showed an intensely hypermetabolic mass lesion filling left maxillary sinus and left nasal cavity (SUVmax 23)
Interpretation
Metastatic lesion at left maxillary sinus and left nasal cavity.
Result
The biopsy from left maxillary sinus showed clear cell carcinoma
Teaching Point
Paranasal sinuses are rare metastatic sites for RCC, but the most frequent primary tumor that metastasizes to paranasal sinuses is the RCC. Approximately 50 cases of nasal recurrences of RCC have been reported in the literature. Tumor involvement of the paranasal sinuses and nasal cavity seems to occur via the hematogenous route through the Batson’s paravertebral venous plexus.
15.6 Case 6: Renal Cell Carcinoma Bone Metastases
History
A 60-year-old male underwent 18F-FDG PET/CT imaging while he was being evaluated for the mass lesion at proximal diaphysis of left humerus.
Findings
Fig. 15.9
Axial CT and PET images showed mass lesion at lower pole of left kidney exhibiting moderately increased FDG uptake (SUVmax 6.8) (a, b), MIP image showed intensely increased FDG uptake at proximal left humerus and focal uptake at proximal diaphysis of right femur (c)
Fig. 15.10
Axial CT and PET images show lytic lesions at cortex of proximal diaphysis of right femur (a, b) and right iliac bone (c, d) both of which showed increased FDG uptake (SUVmax 4.4) (arrows)
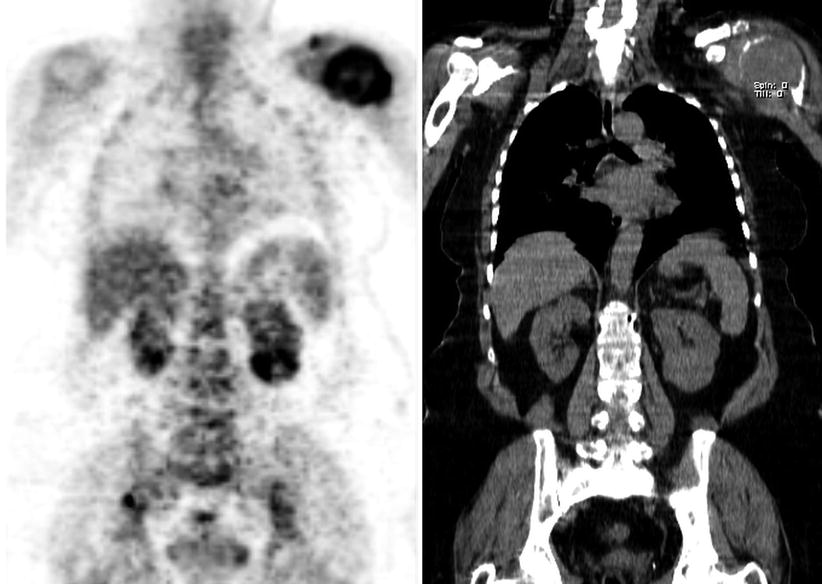
Fig. 15.11
Coronal PET and CT images show mass lesion at lower pole of left kidney with increased FDG uptake
Interpretation
Mass lesion at left kidney was suspicious for malignancy. The hypermetabolism at left proximal humerus, right femur, and right iliac bone was indicating likelihood for metastases.
Result
Biopsy of left humerus lesion revealed giant cell tumor of bone. Patient underwent left nephrectomy and histopathology was RCC.
Teaching Point
One study reported that among all metastatic sites, 18 F-FDG PET/CT is most sensitive for bone metastases of RCC. PET is superior to bone scan in detecting active osseous metastasis of RCC. Sensitivity and specificity 18 F-18 FDG PET/CT reaches up to 100 % for the detection of bone metastases of RCC but there may be false positive findings like benign tumors of bone as in this case.
15.7 Case 7: Renal Cell Carcinoma with Widespread Metastases
History
A 62-year-old male underwent 18F-FDG PET/CT imaging upon detection of a mass lesion at left kidney with anatomical imaging methods.
Findings
Fig. 15.12
Axial CT and fusion images showed mass lesion exhibiting intense FDG uptake, located posterolaterally at left kidney exhibiting moderately increased FDG uptake (SUVmax 19.3); hypodense cystic lesion at right kidney showing no FDG uptake (a, b), hypermetabolic lesion at left scapula extending into muscular structures and left axillary fossa (c, d)
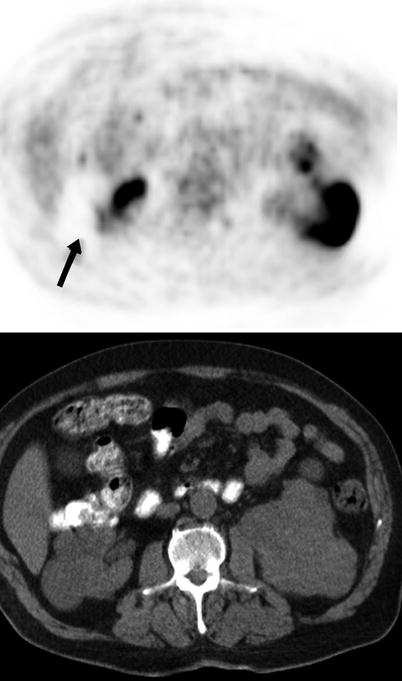
Fig. 15.13




Axial PET and CT images showed hypermetabolic lesion at left kidney and hypodense cystic lesion located at right kidney which shows no FDG uptake (arrow)
Related posts:
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
