Adipocytic tumors
Dedifferentiated liposarcoma
Myxoid/round cell liposarcoma
Pleomorphic liposarcoma
Fibroblastic/myofibroblastic tumors
Fibrosarcoma
Low-grade myxofibrosarcoma
Low-grade fibromyxoid sarcoma
Sclerosing epithelioid fibrosarcoma
So-called fibrohistiocytic tumors
Undifferentiated pleomorphic sarcoma/malignant fibrous histiocytoma (MFH)
Smooth muscle tumors
Leiomyosarcoma
Skeletal muscle tumors
Rhabdomyosarcoma (embryonal, alveolar, and pleomorphic forms)
Vascular tumors
Epithelioid hemangioendothelioma
Angiosarcoma—deep
Tumors of peripheral nerves
Malignant peripheral nerve sheath tumor
Chondro-osseous tumors
Extraskeletal chondrosarcoma (mesenchymal and other variants)
Extraskeletal osteosarcoma
Tumors of uncertain differentiation
Synovial sarcoma
Epithelioid sarcoma
Alveolar soft part sarcoma
Clear cell sarcoma of soft tissue
Extraskeletal myxoid chondrosarcoma
Primitive neuroectodermal tumor (PNET)/extraskeletal Ewing’s tumor
Desmoplastic small round cell tumor
Extrarenal rhabdoid tumor
Undifferentiated sarcoma; sarcoma, not otherwise specified (NOS)
The main indications of FDG–PET/CT in STS are the staging of locally advanced high-grade tumors and the detection of suspected local recurrence.
Rhabdomyosarcoma (RMS) is the most common STS in children and adolescents, accounting for ~5 % of all pediatric cancers and about half of all STS [1]. The tumor can arise anywhere in the body and carries a high risk of locoregional lymph node extension. Survival at 5 years is improved by combining polychemotherapy with local treatment of the primary tumor and its metastases.
18F-FDG–PET/CT provides important additional information in the initial staging of RMS, mainly by evaluating the lymph nodes and metastases, with a significant impact on therapeutic management (Figs. 9.1, 9.2, 9.3, 9.4, 9.5, 9.6, 9.7, 9.8, 9.9, and 9.10). There is also a high prognostic impact of 18F-FDG–PET/CT in the early assessment of the therapeutic response [2, 3].

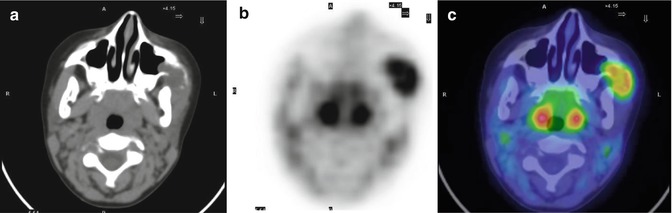
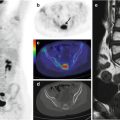
Fig. 9.1
A 6-year-old girl with embryonal rhabdomyosarcoma of the left zygomatic region. Axial CT (a), PET (b), and PET/CT fusion (c) images show large and intense 18F-FDG uptake in the zygomatic arch, masseter and temporal muscles