13
Vascular
Abdominal Aortic Aneurysm (AAA)
Overview
 Defined as >50% dilation of the vessel’s normal size
Defined as >50% dilation of the vessel’s normal size
 90% AAAs are infrarenal
90% AAAs are infrarenal
 Average growth of 3 to 4 mm/yr
Average growth of 3 to 4 mm/yr
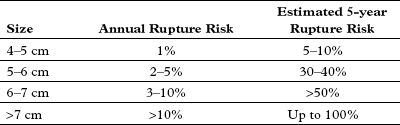
 Rupture risk directly related to size (Laplace’s law)
Rupture risk directly related to size (Laplace’s law)
 Most are a result of atherosclerotic disease
Most are a result of atherosclerotic disease
Normal Vessel Dimensions
 Infrarenal aorta, 1.8 to 3 cm
Infrarenal aorta, 1.8 to 3 cm
 Common iliac, 0.8 to 1.6 cm
Common iliac, 0.8 to 1.6 cm
 External iliac, 0.6 to 1 cm
External iliac, 0.6 to 1 cm
Signs and Symptoms
 Most found incidentally on imaging
Most found incidentally on imaging
 Physical examination is neither sensitive nor specific for asymptomatic aneurysm
Physical examination is neither sensitive nor specific for asymptomatic aneurysm
• Possible findings include pulsatile abdominal mass
 Rupture or impending rupture
Rupture or impending rupture
• Back/abdominal pain + pulsatile abdominal mass = AAA until proven otherwise
• Hypotension/hypovolemic shock
Treatment/Management
 Elective repair if:
Elective repair if:
• Men >5.5 cm, women >4.5 cm
• Expansion >0.5 cm/6 mo
 If not indicated for elective repair, follow up with CT scan or U/S every 6 months
If not indicated for elective repair, follow up with CT scan or U/S every 6 months
RADIOLOGY
 While ultrasound is able to diagnose abdominal aortic aneurysms, CT is more able to define size, involvement of visceral arteries/renal arteries
While ultrasound is able to diagnose abdominal aortic aneurysms, CT is more able to define size, involvement of visceral arteries/renal arteries
Abdominal Aortic Aneurysm (AAA)
 CT Findings (Fig. 13.1)
CT Findings (Fig. 13.1)
• The aneurysm can extend from below the level of the renal arteries to above the aortic bifurcation
• May see mural thrombus
FIGURE 13.1 A–C
A. Kidney
B. Pulmonary hilum
C. Heart
D. Superficial femoral artery
E. Psoas muscle
F. Small bowel
G. Vertebra
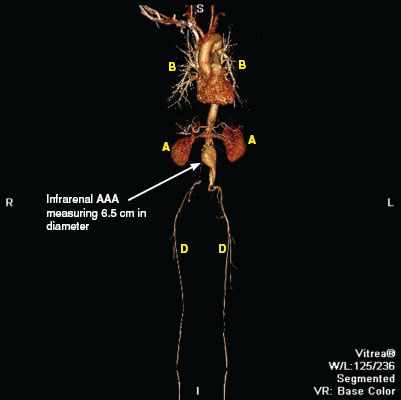
FIGURE 13.1 A
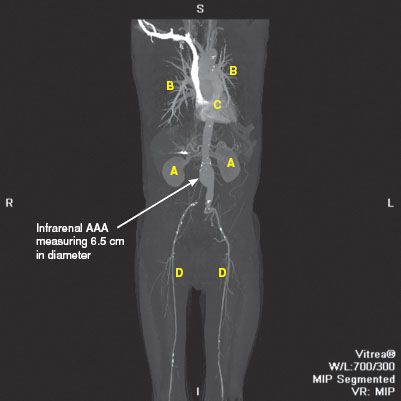
FIGURE 13.1 B
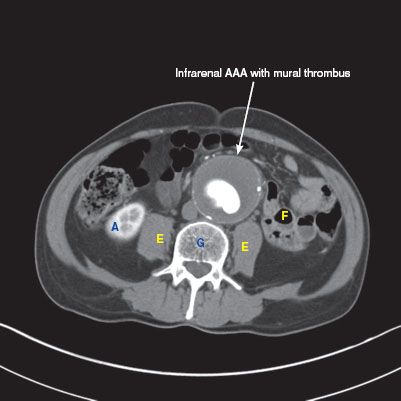
FIGURE 13.1 C
Descending Aortic Aneurysm with Rupture
 CT findings (Fig. 13.2)
CT findings (Fig. 13.2)
• Contrast extravasation from the aorta
• Hemothorax due to blood collecting at the posterior aspects of the lung
FIGURE 13.2 A,B
A. Pulmonary vein
B. Ascending aorta
C. SVC
D. Pulmonary artery
E. Main bronchus
F. Vertebra
G. Liver
H. Kidney
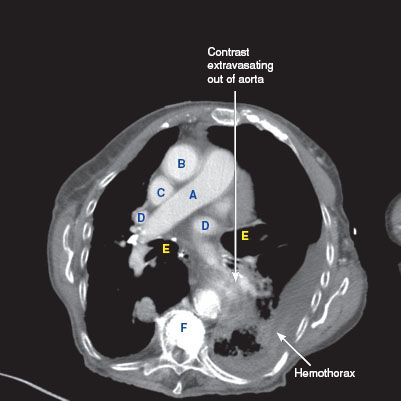
FIGURE 13.2 A
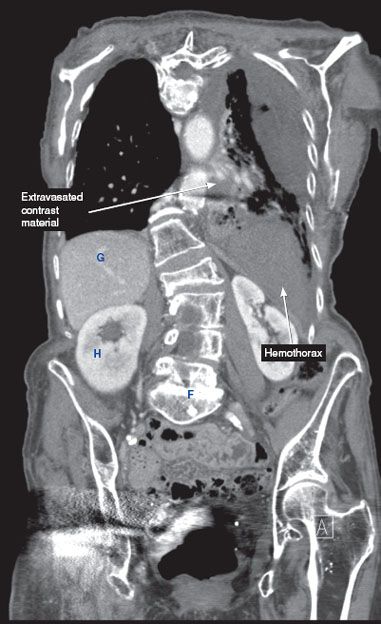
FIGURE 13.2 B
Thoracic Aortic Aneurysm
Overview
 Defined as >50% dilation of the normal diameter
Defined as >50% dilation of the normal diameter
 Managed on the basis of location (ascending vs. arch vs. descending vs. thoracoabdominal)
Managed on the basis of location (ascending vs. arch vs. descending vs. thoracoabdominal)
 True aneurysm (involves all three layers of the arterial wall)
True aneurysm (involves all three layers of the arterial wall)
• Saccular (localized outpouching) versus fusiform (more common)
 False aneurysm
False aneurysm
• Tear in vasa vasorum with bleeding into media layer
 Average expansion rate: Ascending aneurysm 0.7 mm/yr, descending 1.9 mm/yr
Average expansion rate: Ascending aneurysm 0.7 mm/yr, descending 1.9 mm/yr
Etiology
 Nonspecific medial degeneration (result of imbalances between proteolytic enzymes); the most common cause
Nonspecific medial degeneration (result of imbalances between proteolytic enzymes); the most common cause
 Aortic dissection
Aortic dissection
 Genetic disorders: Marfan syndrome, Ehlers–Danlos syndrome, Loeys–Dietz syndrome, familial aortic aneurysmal disease
Genetic disorders: Marfan syndrome, Ehlers–Danlos syndrome, Loeys–Dietz syndrome, familial aortic aneurysmal disease
 Congenital bicuspid aortic valve
Congenital bicuspid aortic valve
 Infectious: Syphilis, Salmonella, Staphylococcus aureus, Staphylococcus epidermidis
Infectious: Syphilis, Salmonella, Staphylococcus aureus, Staphylococcus epidermidis
 Aortitis (chronic inflammation)
Aortitis (chronic inflammation)
Signs and Symptoms
 Typically found incidentally
Typically found incidentally
 May cause localized compression leading to chest pain
May cause localized compression leading to chest pain
 Hoarseness with stretch of left recurrent laryngeal nerve
Hoarseness with stretch of left recurrent laryngeal nerve
 High output heart failure with erosion into SVC
High output heart failure with erosion into SVC
 Distal embolization
Distal embolization
 Symptoms of rupture: Sudden severe chest pain (ascending), back pain (descending), flank and abdominal pain (thoracoabdominal), cardiac tamponade with rupture into pericardium
Symptoms of rupture: Sudden severe chest pain (ascending), back pain (descending), flank and abdominal pain (thoracoabdominal), cardiac tamponade with rupture into pericardium
Treatment
 Medical management
Medical management
• Risk factor reduction (tobacco, hypercholesterolemia, hypertension)
• Blood pressure control
• Screen for other aneurysms since they are often associated with thoracic aortic aneurysm
 Open or endovascular surgical repair if:
Open or endovascular surgical repair if:
• Ascending >5.5 cm
• Descending >6.5 cm
• Repair at 5 cm if concurrent aortic valve replacement or 4.5 cm if undergoing bicuspid aortic valve replacement
• Consider repair at 4 cm if it is associated with aortic regurgitation
RADIOLOGY
 CXR
CXR
• Ascending: Convex shadow right of the cardiac silhouette, loss of the retrosternal space in the lateral view
• Descending: Widening of descending aortic shadow, wall calcifications
Ascending Thoracic Aortic Aneurysm with Dissection (Fig. 13.3)
 CT findings (Fig. 13.3)
CT findings (Fig. 13.3)
• Dissection flap can extend from the aortic root up to the level of the right brachiocephalic artery
• Blood surrounding the ascending aorta
• Fat stranding noted in the pretracheal and aortopulmonary window fat
• Aortic arch vessels are usually fed by the true lumen
FIGURE 13.3 A,B
A. Trachea
B. Sternum
C. Vertebra
D. Brachiocephalic artery
E. Left common carotid artery
F. Left subclavian artery
G. Aortic arch
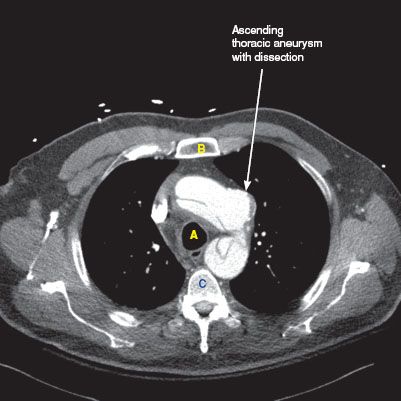
FIGURE 13.3 A
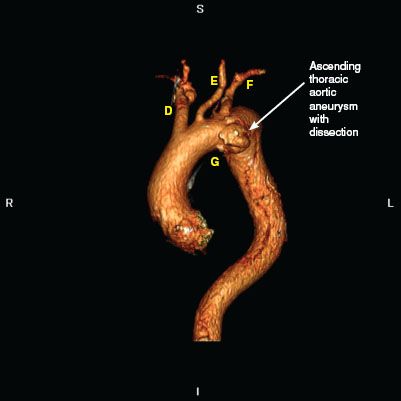
FIGURE 13.3 B
Descending Thoracic Aortic Aneurysm
 Plain film findings (Fig. 13.4)
Plain film findings (Fig. 13.4)
• Convexity of the descending aortic stripe, sometimes with wall calcifications
 CT findings (Fig. 13.4)
CT findings (Fig. 13.4)
• Thoracic aorta diameter exceeding 4 cm is considered aneurysmal
• Can be associated with mural thrombus
FIGURE 13.4 A–C
A. Vertebra
B. Main bronchus
C. Left ventricle
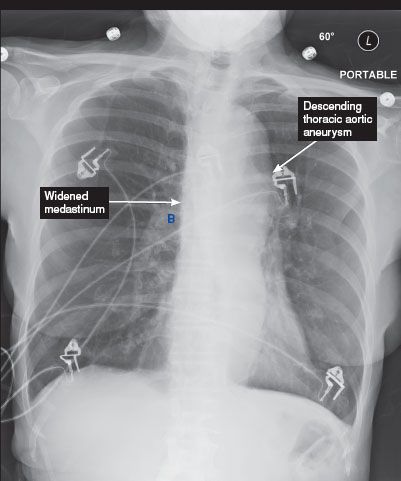
FIGURE 13.4 A
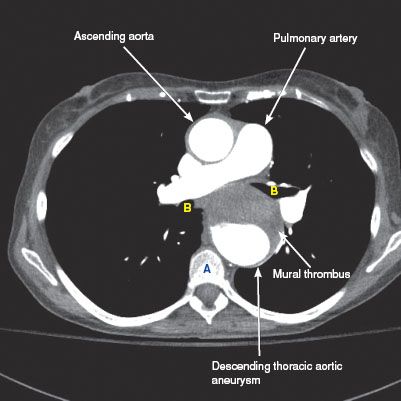
FIGURE 13.4 B




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


