(1)
Department of Radiology, John H Stroger Jr Hospital of Cook County, Chicago, IL, USA
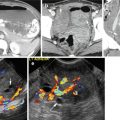
Pulmonary Artery Dissection
Diagnosis
Dissection of the Pulmonary Artery
Imaging Features
1.
Linear dissection flap traversing the main pulmonary artery and extending to the right pulmonary artery
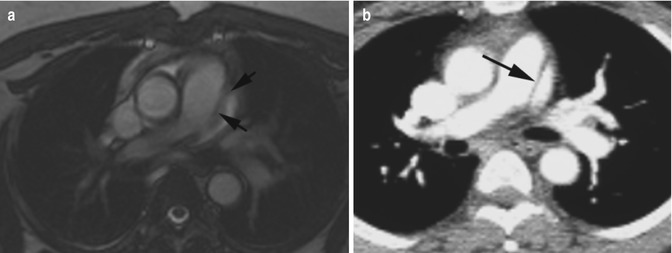
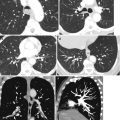
Fig. 3.1
Pulmonary artery dissection. (a) Axial FIESTA cardiac MRI and (b) axial CT show dissection of the main pulmonary artery (arrows). History of hypertension and COPD
Acute Aortic Syndrome
Aortic dissection, intramural hematoma, penetrating atherosclerotic ulcer, and aortic aneurysm rupture
Aortic Dissection
Diagnosis
Acute Aortic Dissection
Imaging Features
1.
Intimal flap separating true and false lumen
2.
Increased attenuation of acute thrombus in false lumen or intramural hematoma in precontrast study
3.
False lumen almost always larger than true lumen
4.
Internal displacement of intimal calcification
5.
Mediastinal, pleural, and pericardial hematoma
6.
Impaired perfusion of end organ either by static obstruction with intimal flap entering origin of the feeding artery or by dynamic obstruction with dissection flap prolapsing and covering the branch vessel ostium
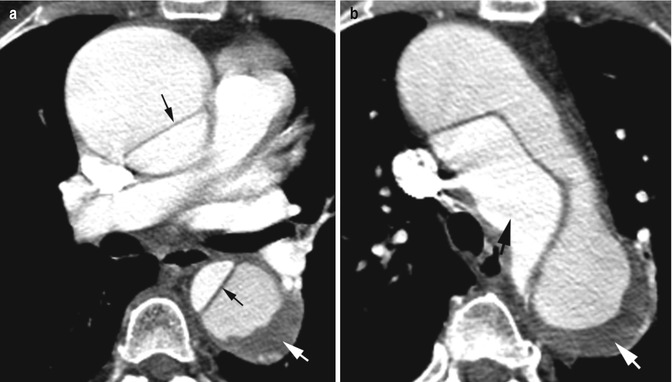
Fig. 3.2
Stanford type A dissection with aneurysmal dilatation of ascending aorta false lumen. Large intramural thrombus in false lumen in the descending aorta. (a, b) Axial CT shows type A dissection with intimal flap (thin black arrow) separating the smaller true lumen from the larger false lumen. In the ascending aorta the false lumen shows aneurysmal dilatation. The descending aorta has thrombus (white arrow) at the periphery of contrast-filled false lumen. True lumen smaller (thick black arrow)
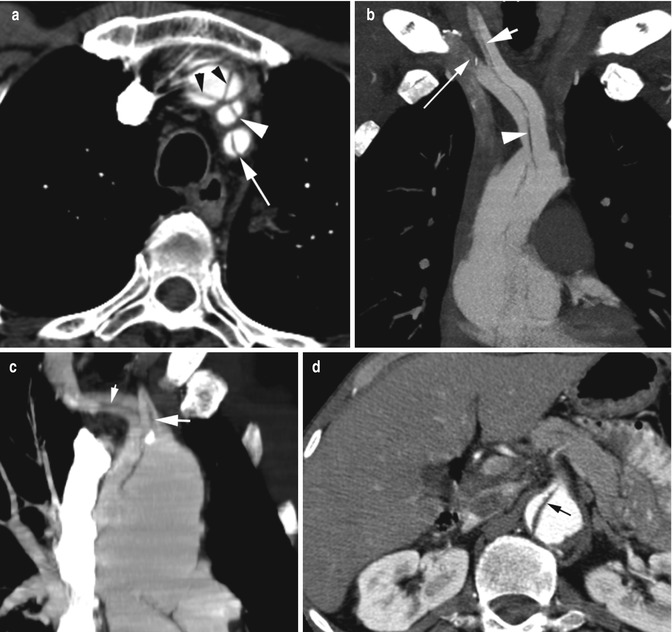
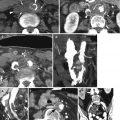
Fig. 3.3
Aortic dissection involving branch vessels. (a) Axial CT of Stanford type A dissection involving left subclavian (arrow), left common carotid (white arrowhead), and brachiocephalic arteries (black arrowheads). Three-channel dissection in the brachiocephalic artery with Mercedes-Benz sign. (b) Coronal MIP image of different patients. Dissection flap (arrowhead) in brachiocephalic artery extending to the right common carotid artery (short arrow) and right subclavian artery (long arrow). (c) Coronal reformatted image of another patient shows dissection flap in the right innominate artery (thin white arrow) and left carotid artery (thick white arrow). (d) Axial CT shows dissection flap extending into the celiac trunk (arrow)
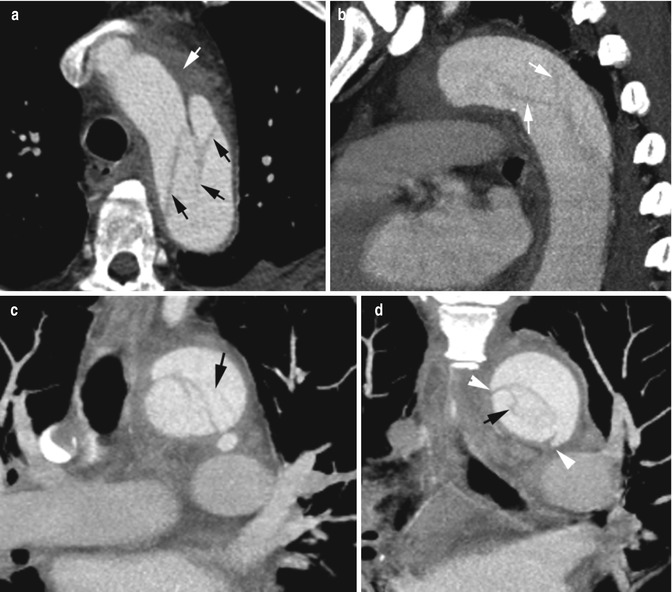
Fig. 3.4
Cobweb and beak sign of false lumen. (a) Axial, (b) sagittal, and (c) coronal reformatted CTs in this type B dissection show thin linear strands of low attenuation in false lumen (black arrows) due to incomplete shearing of the media. Surrounding mediastinal hematoma is seen (white arrow). (d) Coronal reformatted image shows beak sign of false lumen (arrowheads), collagenous medial remnants, and the cobwebs (black arrow)
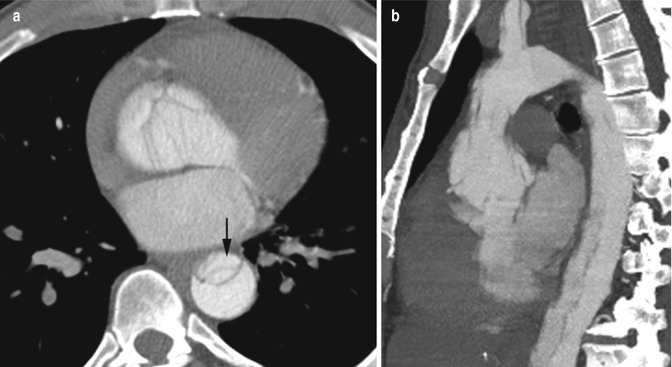
Fig. 3.5
Stanford type A dissection with aneurysm aortic root. History of hypertension and cocaine abuse. At surgery a cyanotic aneurysm was seen of the aortic root with blood in the adventitia and hematoma in the right atrium extending to the right ventricle. (a, b) Axial and coronal reformatted CTs show complex linear low-density intimal tear at root of the aorta from around the annulus. The true lumen is very compressed in the descending aorta (arrow). Aneurysm of the aortic root is best seen at sagittal view
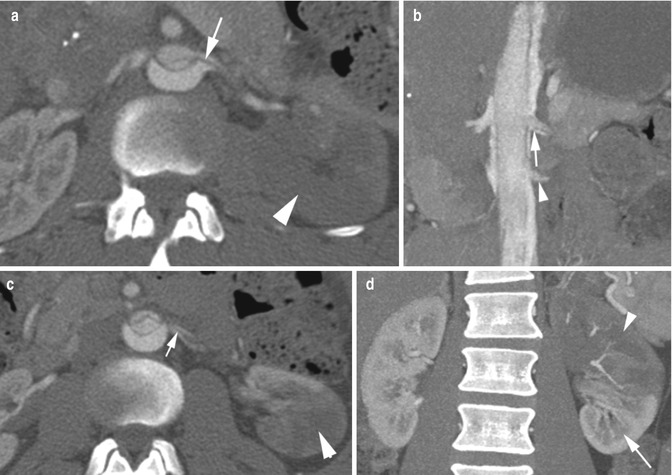
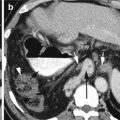
Fig. 3.6
Dissection with static obstruction of the left renal artery. (a, b) Axial CT and coronal reformatted images show intimal flap entering the left renal artery (arrow) with infarction of the upper pole left kidney (large arrowhead). The accessory renal artery (small arrowhead) shows no dissection. (c, d) Axial CT and coronal reformatted images show early branching with good contrast flow in both branches and no dissection of accessory renal artery (short arrow), being connected to the true lumen, supplying the well-perfused lower renal pole (long arrow)
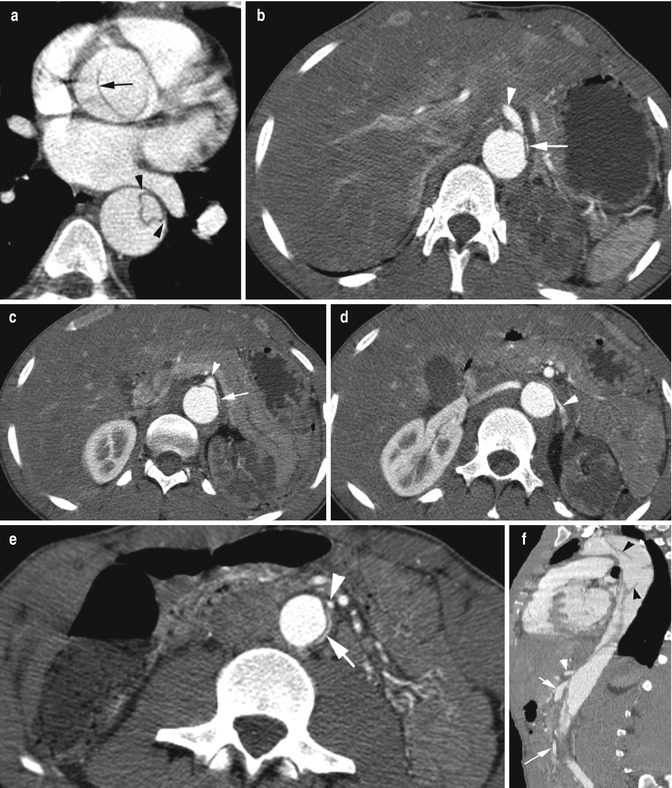
Fig. 3.7
Dynamic obstruction of major branch vessels of the abdominal aorta with ischemia of the liver, bowel, and left renal infarction in Stanford type A dissection. (a) Axial CT shows type A dissection involving root of the aorta. Dissection flap (arrow) in the ascending and descending aorta. Beak sign of false lumen (arrowheads). (b–e) Axial CT images show the celiac trunk, SMA, left renal artery, and IMA (arrowheads) originate from the slit-like true lumen (white arrow) with the origin of these vessels being covered by the dissection flap causing pressure deficit in the true lumen resulting in ischemia of the liver, bowel loops, and frank infarction of the left kidney. (f) Sagittal reformatted image shows wide false lumen with cobwebs (black arrowheads) with the celiac trunk (white arrowhead), SMA (short arrow), and IMA (long arrow) arising from narrow true lumen
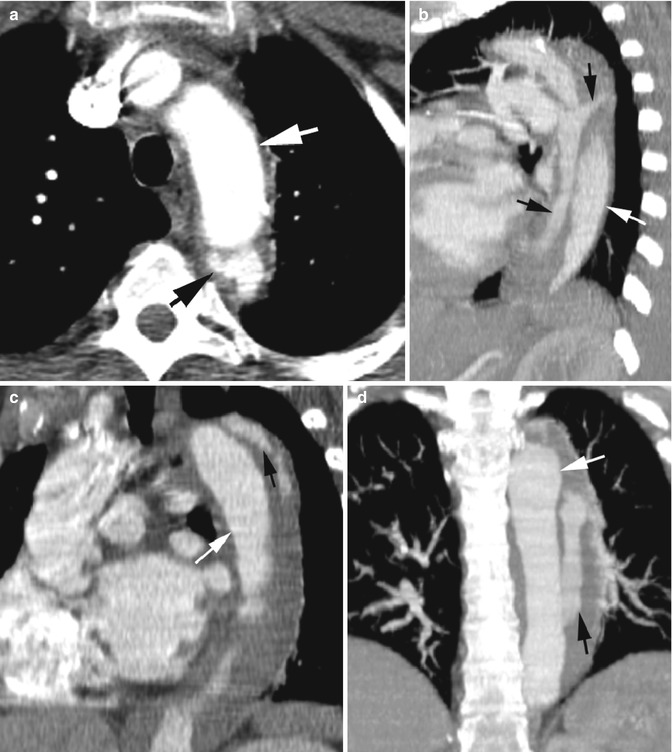
Fig. 3.8
Stanford type B dissection with contrast and thrombus in false lumen. CECT (a) axial and (b) sagittal reformatted images show contrast in false lumen (black arrow) with surrounding thrombus in the descending thoracic aorta spiraling around the true lumen (white arrow). (c, d) Sagittal and coronal reformatted images at different plane show false lumen with central contrast (black arrow) parallel to the true lumen (white arrow)
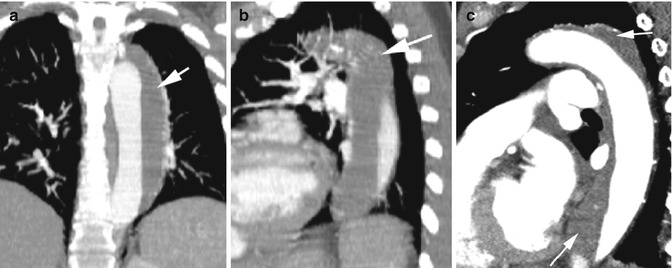
Fig. 3.9
Complete thrombosis of false lumen. Same patient as in Fig. 3.8, CT done 3 years later. (a) Coronal and (b, c) sagittal reformatted images show complete obliteration of false lumen (arrow) by thrombus, giving the appearance of large intramural hematoma
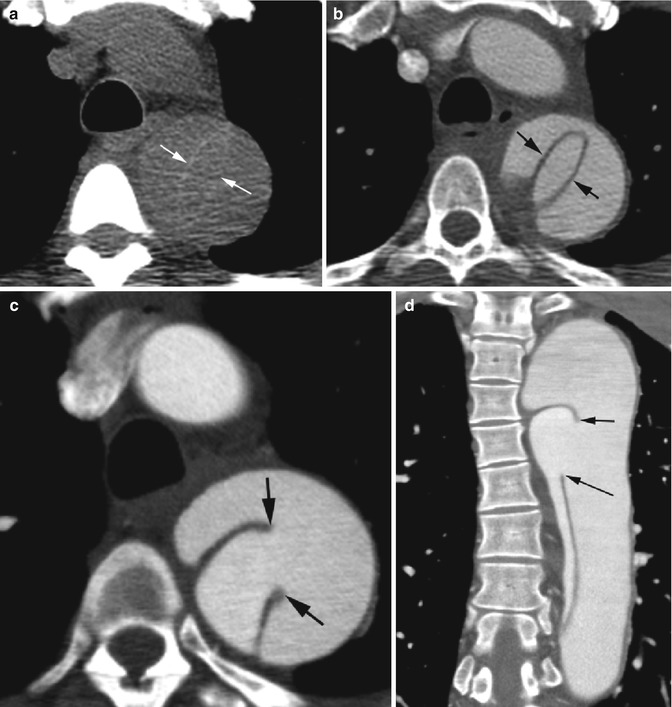
Fig. 3.10
Acute Stanford type B dissection. (a) Precontrast axial CT shows increased attenuation of dissected flap (white arrows). (b) Postcontrast axial CT shows intimal flap (arrows) with similar appearance to precontrast study with central small true lumen surrounded by larger false lumen. (c, d) Axial and coronal reformatted CTs show site of tear (arrows) with smaller true lumen with higher-density contrast
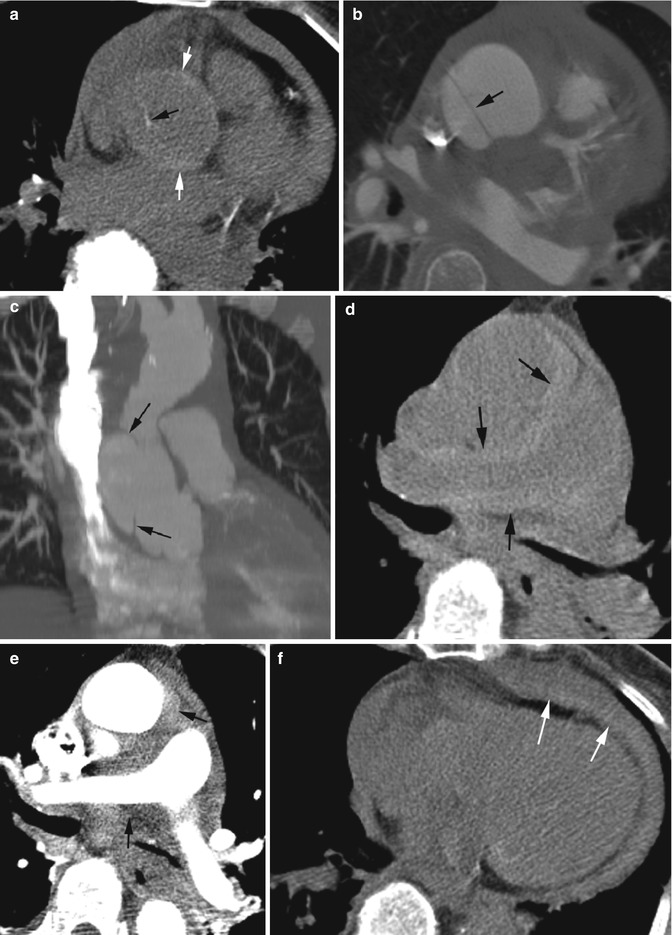
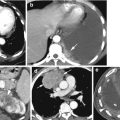
Fig. 3.11
Dissection of the aortic root with displaced intimal calcification. Surgically proven focal Stanford type A dissection of the greater curvature of the ascending aorta near the pulmonary artery with tear into the pericardium. (a) Axial precontrast CT shows faint calcified plaque in the internally displaced flap (black arrow) and faint high attenuation in the aortic rim (white arrow). (b) Intimal flap better seen in postcontrast study, but the calcification is obscured by the contrast (arrow). (c) Coronal reformatted image shows the focal dissection which was about 1.5 cm long at surgery (arrows). (d) Precontrast axial study at higher level than (a) shows high-density hemomediastinum surrounding the aorta and pulmonary artery due to rupture of dissection posteriorly close to the pulmonary artery (arrows). (e) Postcontrast axial CT at same level shows the hematoma (arrow) which is better seen in precontrast CT. (f) Precontrast study shows thin layer of high-density hemorrhagic fluid (arrows) in the pericardium posterior to the low density pericardial fluid. At surgery blood was present at the posterior layers of the pericardium, but the pericardial fluid was serous
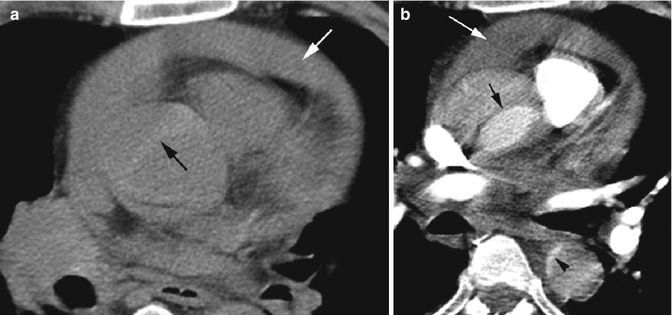
Fig. 3.12




Dissection of the aortic root with hemopericardium. (a) Axial precontrast CT shows acute dissection with high attenuation of intimal flap (black arrow) and high-density hemorrhagic fluid in the pericardium (white arrow). (b) Postcontrast axial study shows the intimal flap (black arrow) separating high-density smaller true lumen from false lumen. Compressed true lumen is seen in the descending aorta with contrast (arrowhead) and also the hemopericardium (white arrow)
Related posts:

Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
