|

Identify the role of diagnostic medical sonography in the assessment of abdominal vascular structures.
Perform sonographic evaluation of the abdominal vascular system.
Describe the patient preparation, equipment considerations, and scanning techniques and Doppler protocols for normal and abnormal abdominal vascular structures.
Identify circulatory anatomy, name the layers of blood vessels, and distinguish the difference between arteries and veins.
Recognize the sonographic appearance and relational anatomy of the abdominal vascular system.
Describe the pathology, etiology, clinical signs and symptoms, and sonographic appearance or aortic pathology to include atherosclerosis, aneurysms, dissection, rupture, inflammatory aneurysms, stenosis, and vascular insufficiency.
Discuss the complications of an aortic graft, including pseudoaneurysms, graft aneurysms, hematomas, abscesses, and occlusions.
Describe the pathology, etiology, clinical signs and symptoms, and the sonographic appearance for venous abnormalities, including vena caval obstruction, tumors, venous enlargement, thrombosis, aneurysm, hepatic venous abnormalities (Budd-Chiari syndrome), and portal venous abnormalities (portal thrombosis and portal venous hypertension).
Formulate a list of differential diagnosis based on correlating the patient’s clinical history, laboratory values, results of related diagnostic procedures, and the sonographic tissue characteristics.
Identify technically satisfactory and unsatisfactory sonographic examinations of the vascular system.
posterior, a short distance medial, and then superior to form the ascending aorta. It then curves lateral and posterior to form the aortic arch. As the aorta completes its curve at the arch, it begins to descend inferiorly into the chest. This portion, the descending aorta, soon gives rise to the thoracic aorta. Once the aorta penetrates the diaphragm, it is termed the abdominal aorta until it bifurcates into the common iliac arteries prior to entering the pelvic cavity. It is the abdominal aorta that is most accessible to sonographic examination (Fig. 6-2).
 FIGURE 6-1 Segments of the aorta. The common reference segments, ascending, arch, descending, thoracic, and abdominal aorta can be identified on the illustration. |
 FIGURE 6-2 Major branches. An anterior illustration of the abdominal aorta showing the anatomic location of its major branches. |
 FIGURE 6-3 Relationships. The abdominal aorta and its branches are illustrated along with representative sonograms. A: The level of the transverse section is made through the celiac trunk. B: The level of the transverse section is made through the pancreas. C: The level of a longitudinal section is made through the upper aorta. (Reprinted with permission from Moore KL, Agur AMR, Dalley AF II. Essential Clinical Anatomy. 5th ed. Wolters Kluwer Health; 2015:191. See page 191 of resource book.) |
 FIGURE 6-4 Longitudinal aorta. A: The longitudinal plane through the proximal abdominal aorta (Ao) demonstrating the celiac axis (CA) and superior mesenteric artery (SMA). The liver (L) is anterior to the aorta, and the vertebral bodies (VB) are posterior to the aorta. B: With the patient positioned in a right lateral decubitus, the longitudinal plane demonstrates the bifurcation of the aorta into the right common (R) and left common (L) iliac artery at the level of the umbilicus. |
more comprehensive imaging of the iliac arteries is accomplished by placing the transducer in the iliac fossa and angling medially with the scan plane oriented approximately 45 degrees from midline. Demonstration of the length of the iliac arteries is thus achieved. At times, successful imaging of the iliac arteries requires a distended urinary bladder. In this case, the transducer is placed in the midline of the pelvis and oriented 45 degrees from midline. Lateral angulation will result in visualization of the iliac vessels.
 FIGURE 6-5 Transverse and coronal planes through the aorta (Ao). A: The transverse plane at the level of the celiac axis (CA) is the hepatic artery (HA) and splenic artery (SA). B: The transverse plane at the level of the branching right renal artery (RRA) and left renal artery (LRA) off of the Ao can be seen with its relationship to the superior mesenteric artery (S). C: The coronal plane demonstrating the renal artery origins. This sonographic appearance is referred to as the “banana peel.” D: The transverse image demonstrating the left renal vein (LRV) being compressed (cursors) between the A and superior mesenteric artery (SMA), which is known as the “nutcracker phenomenon.” E: Transverse image of the Ao and inferior mesenteric artery (I). IVC, inferior vena cava. |
in which the IVC expands during this maneuver. With suspended inspiration, the IVC expands because of increased intrathoracic pressure and decreased blood flow into the heart. During the Valsalva maneuver, the IVC collapses because of the increased abdominal pressure associated with this technique.8,9
 FIGURE 6-6 Normal inferior vena cava (IVC). A: A longitudinal sonogram through the IVC demonstrating the hockey stick configuration as the vessel as it nears the right atrium (RA). B: Image displaying the relationship of the IVC draining into the RA. PV, portal vein. (A: Courtesy of Philips Medical System, Bothell, WA.) |
 FIGURE 6-7 Abdominal veins. The most often sonographically visualized veins and their relationships are depicted on the illustration of the inferior vena cava, its tributaries, and the formation of the portal venous system. |
 FIGURE 6-8 Transverse sections. A: A transverse plane through the liver showing the right hepatic vein (R), middle hepatic vein (M), and left hepatic vein (L), and they drain into the inferior vena cava (IVC). B: A transverse plane through the right kidney (RK) demonstrating the right renal vein (RV) as it drains into the IVC. |
 FIGURE 6-9 Portal system. A: Transverse sonogram through the upper abdomen showing the splenic vein (SV) as it converges with the superior mesenteric vein to form the portal confluence (PC), the beginning of the portal vein. B: The longitudinal sonogram demonstrating the superior mesenteric vein (SMV) as it courses parallel to the inferior vena cava (IVC) which is seen posterior. C: An oblique plane through the right upper quadrant visualizes the portal vein (PV) as it enters the liver and branches into the right portal vein (RPV) and the left portal vein (LPV). Ao, aorta; LRV, left renal vein. (C: Courtesy of Philips Medical System, Bothell, WA.) |
branch artery. Detection of a hemodynamically significant stenosis is discussed in detail later in this chapter.
 FIGURE 6-10 Relationships. Collective illustration of the major branches of the aorta, inferior vena cava, and the portal system helps visualize the abdominal vascular and organ relationships. |
TABLE 6-1 Relational Anatomy | ||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||
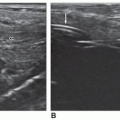
 FIGURE 6-11 Arteriosclerotic aorta. Diffuse plaque (arrows) with minimal acoustic shadowing can be seen in the longitudinal sonogram through the distal portion of an aorta. (Image courtesy of Philips Medical System, Bothell, WA.) |
 FIGURE 6-12 Aneurysms. The illustration presents three types of true aneurysms: (A) saccular, (B) fusiform, circumferential, and (C) dissecting. |
in the evaluation of suspected aortic aneurysm and can be used to monitor the growth of aneurysms over time.23 However, there are some important considerations to keep in mind to avoid misdiagnosis of an aneurysm. Tortuosity may make the aortic diameter appear larger than it is. This occurs when the plane of imaging is not truly perpendicular to the aortic walls. Therefore, careful observations should be made of the aortic curvature in these instances to avoid misrepresentation of a tortuous aortic segment as an aortic aneurysm. Excessive air in the abdomen or obesity may obscure the distal aorta and iliac vessels and render some aneurysms invisible. Lymphadenopathy may also confound the picture.21,22
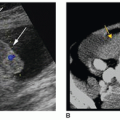
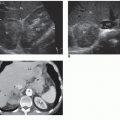
 FIGURE 6-13 Aneurysms. A: The longitudinal plane sonogram demonstrating a normal caliber aorta (Ao). B: The longitudinal section demonstrating an abdominal aortic aneurysm with mural thrombus (MT). C: On the same patient, the transducer is turned 90 degrees from the longitudinal plane for a transverse image of the aneurysm. The mural thrombus has the appearance of a crescent sign because the thrombus has begun to liquefy. D: Doppler instrumentation aids in proving blood flow as well as visualizing subtle mural thrombus compared to the total size of the aneurysm. E: Longitudinal image demonstrating juxtarenal and infrarenal aortic aneurysms. F: The sonogram obtained with a coronal plane demonstrating the renal artery origins (arrows) proving infrarenal aneurysm. G, H: These transverse sonograms display an abdominal aortic aneurysm. G: A transverse sonogram demonstrates the anechoic crescent sign (arrows) due to the area within the thrombus that has liquefied. H: A transverse sonogram with color Doppler provides evidence of blood flow as well as the residual lumen compared to the total size of the aneurysm. On both sides of the vessel, refraction creates shadowing artifacts (arrows). (G and H: Courtesy of Philips Medical System, Bothell, WA.) |
 FIGURE 6-14 Aneurysm classifications. The three types of aortic dissections illustrated were categorized by DeBakey. |
 FIGURE 6-15 Dissecting aneurysm. A: A transverse sonogram of the aorta demonstrating a linear flap (arrow) with the arterial lumen consistent with dissection. B: On a longitudinal sonogram through an abdominal aorta, a thin linear echo flap (carets) is noted paralleling the anterior wall. C: The Doppler interrogation showing narrowing of an aorta flow with increased speed. (A: Courtesy of Jill Langer, MD, Hospital of University of Pennsylvania, Philadelphia, PA. B and C: Courtesy of Philips Medical System, Bothell, WA.) |
organs and structures.12 Other findings suggestive of aortic aneurysm rupture include irregular intra-abdominal fluid collections in association with aortic aneurysm and diffuse irregular hypoechoic areas near an aortic aneurysm.
aneurysms to rupture, early detection is important so that prompt treatment can be obtained.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


