Figure 11.1.1
Omphalocele containing bowel. A: Transverse image of fetal abdomen (arrowheads) demonstrating well-circumscribed mass (arrows) protruding anteriorly at the umbilical cord insertion. B: Image in same fetus showing heterogeneity of the protruding mass (calipers), indicating that it contains only bowel. C: Transverse image of abdomen (arrowheads) in another fetus showing large omphalocele (arrows) containing only bowel.
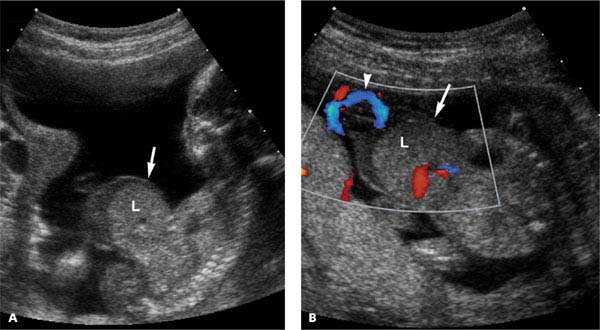
Figure 11.1.2
Omphalocele containing liver. A: Sagittal image of fetus demonstrating large omphalocele (arrow) containing a region of homogeneous tissue representing liver (L). B: Color Doppler image of large omphalocele (arrow) showing vessels in the herniated portion of the liver (L). Umbilical vessels (arrowhead) are seen inserting into the omphalocele sac.
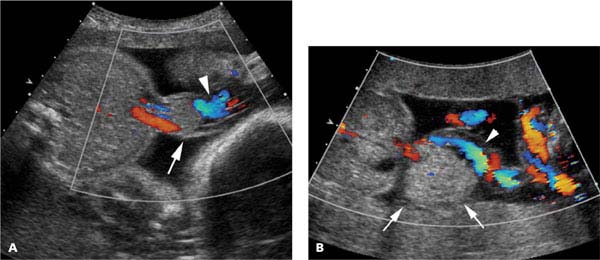
Figure 11.1.3
Umbilical vessels coursing through omphalocele. A: Transverse image with color Doppler of abdomen in 29-week fetus with Beckwith–Wiedemann syndrome and small omphalocele (arrow) showing blood flow through umbilical vessels (arrowhead) coursing through and out of the omphalocele with color Doppler. B: Sonogram with color Doppler in same fetus as Figure 11.1.1(C) showing umbilical vessels (arrowhead) coursing through large omphalocele (arrows).
11.2. Gastroschisis
Description and Clinical Features
Gastroschisis is a paraumbilical defect in the anterior abdominal wall through which intra-abdominal contents, usually bowel, herniate into the amniotic cavity. Unlike an omphalocele, the herniated tissue is free-floating in the amniotic fluid, not contained within a membrane. The defect is usually to the right of the umbilicus. Gastroschisis tends to affect young mothers more often than older mothers. Aneuploidy is uncommon. Other anomalies are present in approximately 25% of cases, many of which, such as malrotation, are related to the gastrointestinal tract.
The prognosis for gastroschisis is fairly good, especially if the amount of herniated bowel is small. Infants require surgery shortly after birth and many have gastrointestinal and infectious complications after the repair. Long-term gastrointestinal complications, including malabsorption, are common.
Sonography
In the second trimester, gastroschisis typically appears as an irregular mass of tissue anterior to the abdomen on one side of the umbilical cord insertion (Figure 11.2.1). The amount of bowel herniated may increase as pregnancy progresses, and the herniated bowel loops may progressively dilate (Figure 11.2.2). Partial bowel obstruction may cause dilation of the stomach (Figure 11.2.3) and/or intra-abdominal loops of bowel (Figure 11.2.4), as well as polyhydramnios. Rarely, the liver or other abdominal organs may herniate through the gastroschisis defect.
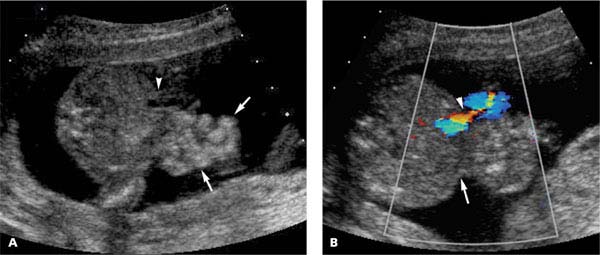
Figure 11.2.1
Gastroschisis. A: Transverse image of abdomen demonstrating loops of free-floating bowel (arrows) protruding from anterior abdominal wall, adjacent to cord insertion (arrowhead). B: Color Doppler image demonstrating umbilical cord insertion (arrowhead) adjacent to defect (arrow) of gastroschisis.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


