Discrete intramural nodules appear T2 hyperintense and hypointense on T1WI and T1WI C+
Thickened gallbladder wall and intramural nodules may show signal drop-out on out-of-phase images
Thickened wall often demonstrates delayed enhancement on T1WI C+
• US: Hypoechoic nodules or bands within thickened GB wall
Gallstones, sludge, echogenic intraluminal debris
PATHOLOGY
• Mucosal ulceration or rupture of Rokitansky-Aschoff sinuses → extravasation of bile into GB wall → phagocytosis of bile lipids → inflammation and xanthoma cell formation
• Gallstones always present and may play causative role
CLINICAL ISSUES
• Symptoms most often similar to acute cholecystitis, but can be chronic and mimic malignancy
• More common in females during 6th or 7th decade of life
• Only definitive treatment is cholecystectomy
(Left) Resected GB shows marked wall thickening and an intramural abscess . A portion of the adjacent liver was resected because of the high intraoperative suspicion of GB cancer. Pathology revealed xanthogranulomatous cholecystitis (XGC).
(Right) Axial CECT shows a thickened wall of the gallbladder, especially the fundus , with an indistinct border with the liver. While the appearance was concerning for gallbladder cancer, this was found to be XGC at cholecystectomy.
(Left) Axial CECT of a patient with RUQ pain shows marked irregular GB wall thickening , intramural low attenuation , and several pericholecystic collections . Low-attenuation intramural nodules in XGC are due to either abscesses or xanthogranulomas.
(Right) Axial NECT in a patient with chronic abdominal pain shows a distended, thick-walled gallbladder exhibiting indistinct margins with the liver . While this was worrisome for carcinoma, XGC was confirmed at surgery.
 Pericholecystic fluid and inflammatory change ± fistulous tracts, abscesses, contained perforation, etc.
Pericholecystic fluid and inflammatory change ± fistulous tracts, abscesses, contained perforation, etc.





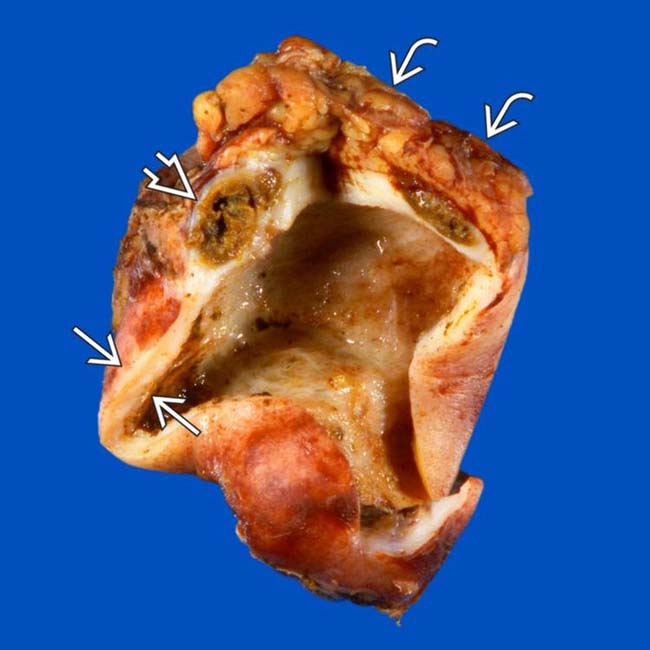
 and an intramural abscess
and an intramural abscess  . A portion of the adjacent liver
. A portion of the adjacent liver  was resected because of the high intraoperative suspicion of GB cancer. Pathology revealed xanthogranulomatous cholecystitis (XGC).
was resected because of the high intraoperative suspicion of GB cancer. Pathology revealed xanthogranulomatous cholecystitis (XGC).
 , with an indistinct border with the liver. While the appearance was concerning for gallbladder cancer, this was found to be XGC at cholecystectomy.
, with an indistinct border with the liver. While the appearance was concerning for gallbladder cancer, this was found to be XGC at cholecystectomy.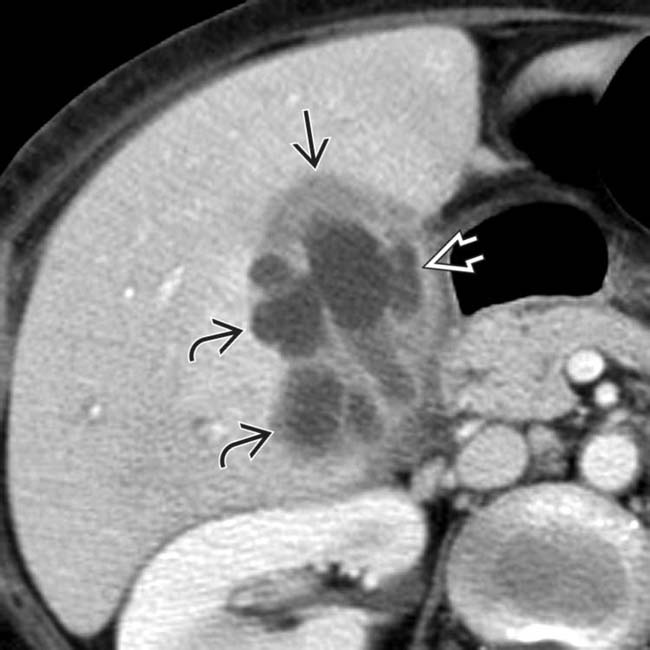
 , intramural low attenuation
, intramural low attenuation  , and several pericholecystic collections
, and several pericholecystic collections  . Low-attenuation intramural nodules in XGC are due to either abscesses or xanthogranulomas.
. Low-attenuation intramural nodules in XGC are due to either abscesses or xanthogranulomas.
 . While this was worrisome for carcinoma, XGC was confirmed at surgery.
. While this was worrisome for carcinoma, XGC was confirmed at surgery.




 Low-attenuation intramural nodules and bands corresponding to foamy cell infiltrate and areas of necrosis/abscess
Low-attenuation intramural nodules and bands corresponding to foamy cell infiltrate and areas of necrosis/abscess Pericholecystic fluid, inflammatory change, and induration ± fistulous tracts, abscesses, contained perforation, etc.
Pericholecystic fluid, inflammatory change, and induration ± fistulous tracts, abscesses, contained perforation, etc.
















