Case presentation
A 2-year-old female presents to the emergency department with wheezing and cough. The family states that she has had mild fever to 100.1 degrees Fahrenheit for the past 2 days. There has been no vomiting or diarrhea. She has been taking oral fluids well and is otherwise behaving at her baseline. Her physical examination reveals a well-appearing child in no respiratory distress. She has nasal congestion and some inspiratory wheezing at the upper lung fields.
The parents state they are frustrated and “want something for the cough and wheezing,” which has been intermittently present “as long as they can remember” and seems to get worse when the child has upper respiratory infections. They have seen their primary care provider multiple times for these symptoms and have been told the child has reactive airway disease. Albuterol was prescribed, but the family states that this medication is not helping the child’s wheezing. Multiple courses of oral steroids have been prescribed and the child has been given a fluticasone inhaler but this too has had no impact on her symptoms.
Imaging considerations
Plain radiography
Two-view chest radiography (anteroposterior [AP] and lateral views) is the first-line imaging modality in patients with respiratory symptoms and serves as a helpful screening examination for vascular rings. On AP views, one should evaluate the relationship of the aorta relative to the trachea, determining the side of the aortic arch, and one should evaluate for tracheal narrowing on the lateral view, which may suggest compression from a vascular ring or sling. A right-sided aortic arch may be associated with a variety of cardiac lesions (up to 50% of patients), including persistent truncus arteriosus, pulmonary atresia with ventricular septal defect, and tetralogy of Fallot. Anomalies of the aortic arch and the resulting aortic arch branching pattern and position of the ductus arteriosus will determine whether the vasculature forms a complete vascular ring, producing clinical symptoms. Two branching patterns of a right-sided aortic arch, a retroesophageal aberrant left subclavian artery (65%) and mirror-image branching (35%), can be seen, with the mirror-image branching type more commonly associated with congenital heart disease. A left-sided aortic arch with a an aberrant right subclavian artery may also be associated with congenital heart disease, but this configuration will form an incomplete vascular ring, thus producing fewer clinical symptoms compared to a right-sided arch configuration.
Findings suspicious for a vascular ring on AP images include a right-sided aortic arch, abnormal tracheal indentation, and a right descending aorta, whereas lateral radiographic findings include increased retrotracheal opacity, tracheal narrowing, and anterior tracheal bowing. , If a double aortic arch is present, the aorta may not be easily visualized. , Unilateral hyperinflation of the right lung, tracheal narrowing, and an atypical orientation of main bronchi suggest a pulmonary artery sling. Chest radiography has the advantage of availability, rapidity, and minimal ionizing radiation exposure. However, more advanced imaging techniques become necessary if an abnormality is suspected.
Barium esophagography
Barium esophagram has historically been utilized to evaluate for suspected vascular rings. An esophagram is useful in that it demonstrates relatively characteristic extrinsic impressions on the esophagus from anomalous vessels that contribute to a vascular ring. The presence of a double aortic arch may be seen with bilateral aortic arch and posterior crossing vessel indentations upon the esophagus. With other vascular rings, depending on the location and orientation of the vascular ring, different degrees of esophageal indentation may be seen. , Barium esophagography can also be used to evaluate other etiologies of feeding difficulties, such as gastroesophageal reflux and tracheoesophageal anomalies. This modality, however, requires expertise in performance of the study and interpretation of imaging results and includes exposure to ionizing radiation. Availability may be institution dependent. While the diagnosis of a vascular ring can be made with this modality, barium esophagography does not directly visualize the vascular ring and additional imaging is usually required. A well-performed negative barium esophagram can exclude a vascular ring, with the exception of an aberrant innominate artery. , Abnormal barium esophagography should be followed by either computed tomography (CT) or magnetic resonance imaging (MRI). These cross-sectional imaging modalities will provide direct imaging of the vasculature, which is critical in determining if a surgical lesion is present and for planning appropriate operative repair.
Computed tomography
CT angiography with intravenous contrast is an excellent imaging modality to identify vascular anomalies of the aortic arch and pulmonary arteries and can depict resulting vascular rings. , , , CT is often obtained as part of the presurgical planning process.
Magnetic resonance imaging/magnetic resonance angiography (MRA)
This imaging modality is very useful for imaging mediastinal vascular structures and can provide anatomic information with or without the use of intravenous contrast. MRI and MRA are also used as part of presurgical planning. , ,
CT versus MRI
CT and MRI have the same sensitivity for detecting vascular rings. CT has the advantage of availability, rapidity, and not requiring sedation in most cases. This modality also has excellent spatial resolution and multiplanar and three-dimensional reconstruction capabilities, can be used for virtual bronchoscopy, and can evaluate the vasculature, airways, and, to some degree, the esophagus. , CT angiography involves the use of ionizing radiation and intravenous contrast material. MRI can visualize the relationship of the vasculature and trachea very well, in addition to detecting airway anomalies, and can also provide evaluation of the heart and any associated anomalies; intravenous contrast agents are not always utilized for MRI and their use may be institution dependent. , , MRI, though, is limited by the need for sedation and availability, which may be institution dependent.
Which modality, CT or MRI, is employed may be dependent on the previously-mentioned factors, in addition to subspecialty preference. Consultation with pediatric cardiology or cardiothoracic surgery and pediatric radiology prior to obtaining advanced imaging is appropriate.
Ultrasound (US)
Patients with a diagnosis of vascular ring should have echocardiography, since 12% of patients with a vascular ring have associated congenital heart disease. Prenatal US has been reported to be useful in screening for vascular rings. Once a vascular ring is suspected, detailed attention may be provided to the relationship of the aortic arches, ductal arches, and the trachea. , Postnatal US can be used to identify the laterality of the aortic arch and aortic branching patterns. , US has the advantage of lacking ionizing radiation, lacking the need for sedation, and general availability. However, ultrasonography is less effective at visualization for vascular anomalies in older patients (due to a decreasing size of the thymic acoustic window with increasing age). ,
Imaging findings
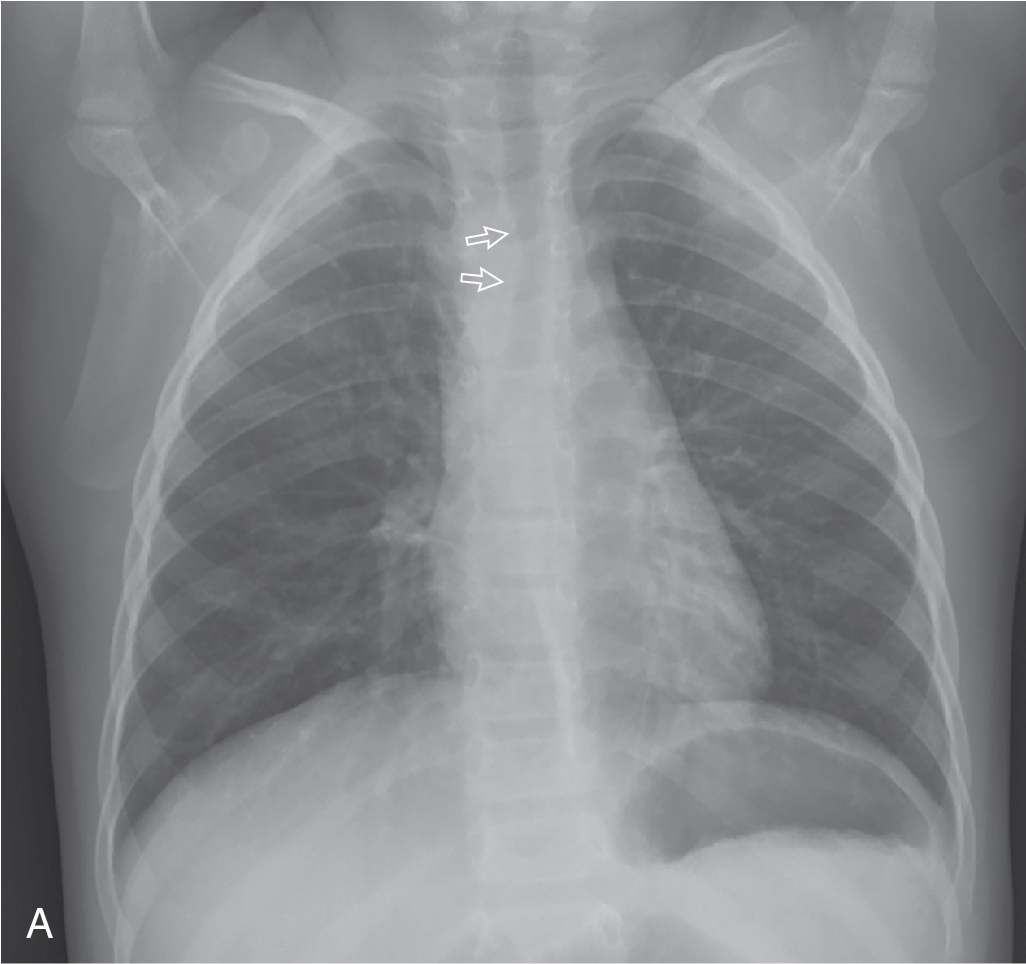
The patient has an acute illness that is consistent with a viral infection. However, due to the history of chronic wheezing and cough, the decision was made to obtain plain radiography of the chest. These images are provided here. The trachea normally buckles away from the side of the aortic arch. There is leftward tracheal deviation consistent with a right aortic arch. There is no focal consolidation or effusion; the heart size and pulmonary vascularity are normal ( Fig. 13.1 ).