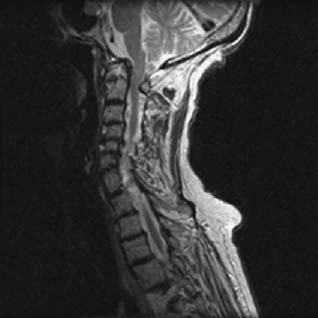
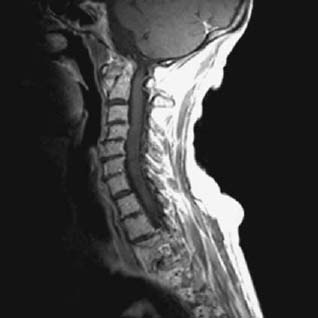
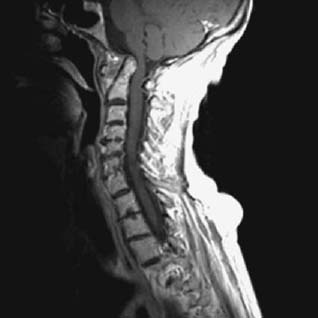
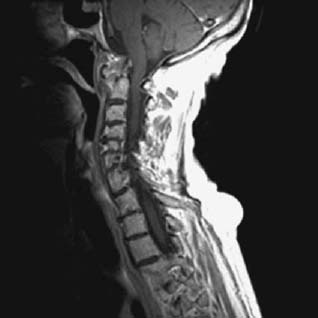
CASE 103 Hema N. Choudur, Anthony G. Ryan, and Peter L. Munk A middle-aged woman with known rheumatoid arthritis presented with sudden onset neck pain and instability. On examination, restricted motion of the neck was noted. No neurological deficit was present. Figure 103A Figure 103B Figure 103C Figure 103D Initial cervical spine radiographs were unremarkable, but clinical instability indicated flexion and extension views. The extension view is unremarkable (Fig. 103A); however, increased distance between the posterior margin of the atlas and the anterior margin of the dens is evident on the flexion view (Fig. 103B), findings suggestive of atlantoaxial instability (AAI). Subsequent MRI (Figs. 103C–103E, T2 and Figs. 103F–103H, T1 postgadolinium) reveals an avidly enhancing pannus eroding the anterior margin of the odontoid process on its left side. The spinal cord is compressed posteriorly. Further cord impingement is evident inferiorly secondary to cervical spondylosis. Figure 103F Figure 103G Figure 103H AAI secondary to rheumatoid pannus. In the pediatric population, there are several potential causes of AAI: Excessive movement between C1–C2 may be either bony or ligamentous. A high index of clinical and radiologic suspicion is required, and although initial cervical radiographs may be unremarkable, suspected instability should be investigated further by dynamic cervical spine views or CT with reformats to demonstrate the instability.
Atlantoaxial Instability
Clinical Findings


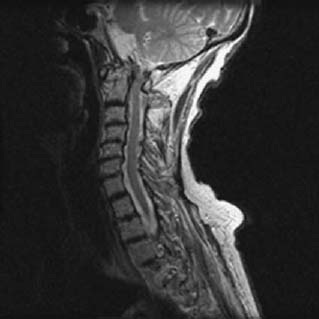
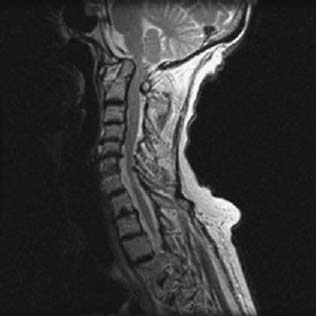
Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


