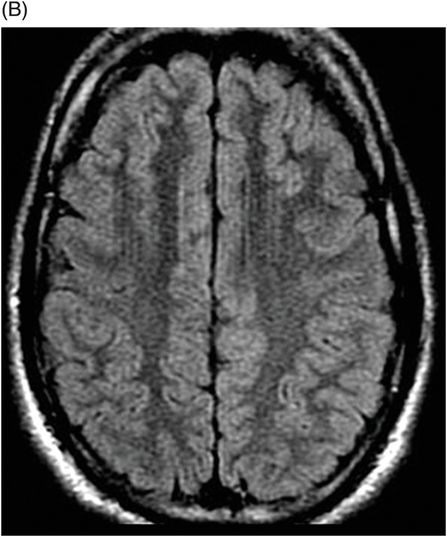
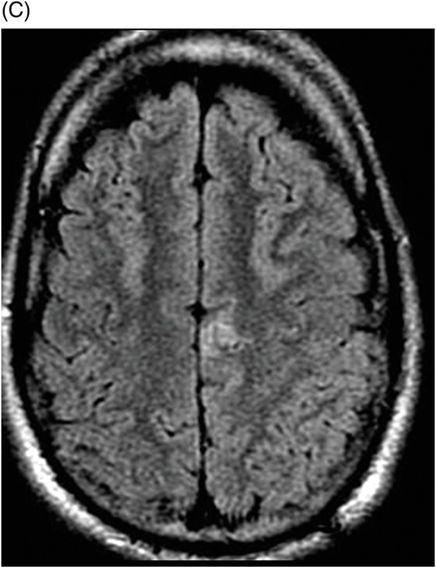
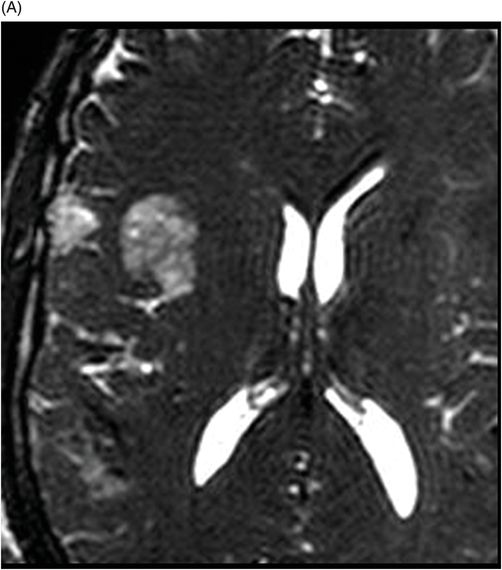
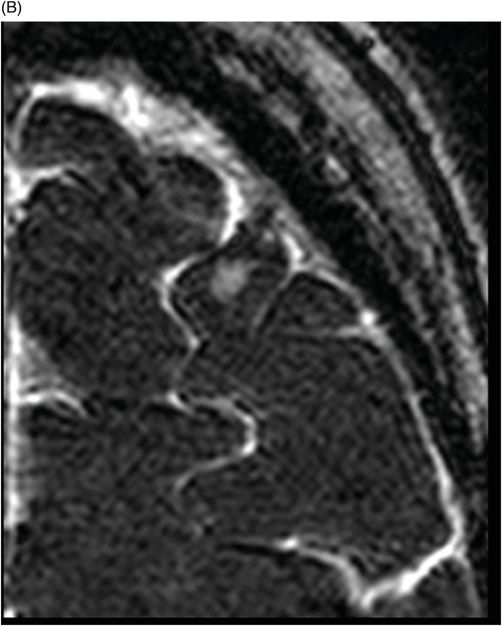
(A) Axial 3D-CISS through the right frontal operculum, (B) through the left middle frontal gyrus, and (C) through the left superior frontal gyrus.
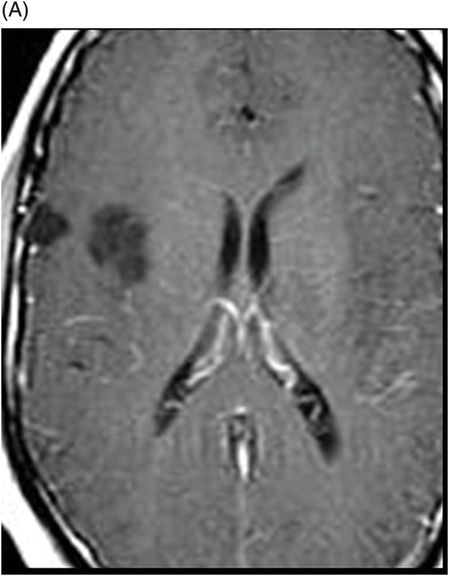
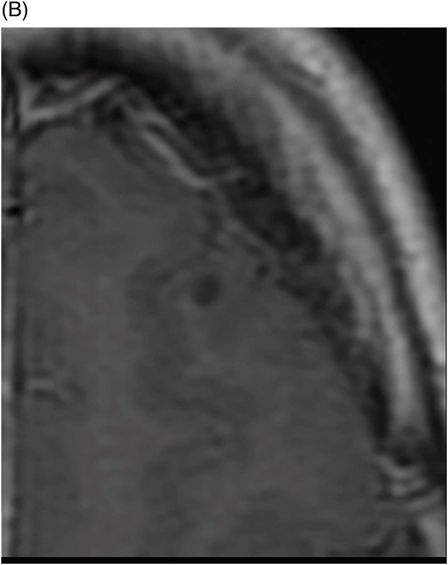
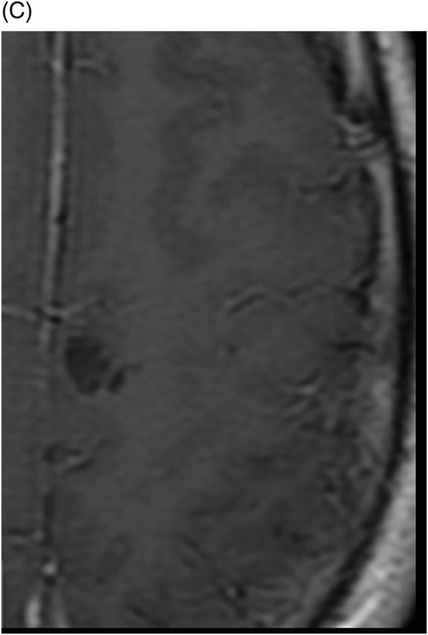
(A) Axial contrast-enhanced T1WI through the right frontal operculum, (B) through the left middle frontal gyrus, and (C) through the left superior frontal gyrus.
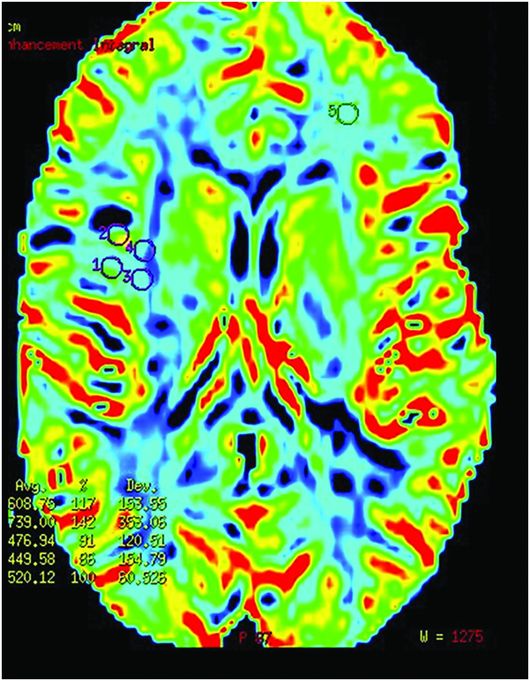
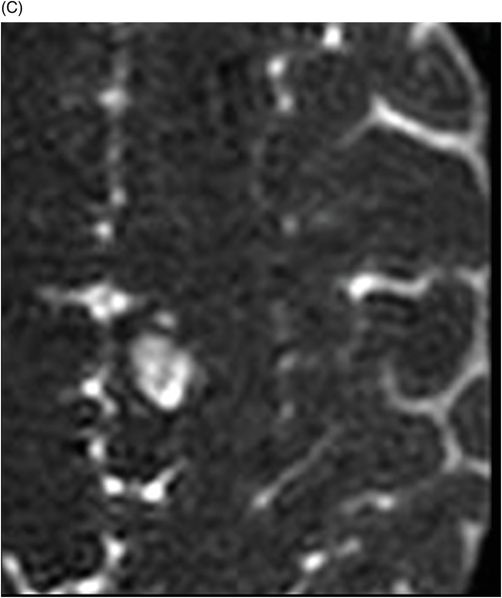
T2 Perfusion-DSC through the large lesion in the right frontal operculum.
Multifocal Dysembryoplastic Neuroepithelial Tumor
Primary Diagnosis
Multifocal dysembryoplastic neuroepithelial tumor
Differential Diagnoses
Low-grade astrocytoma
Ganglioglioma
Angiocentric glioma
Oligodendroglioma
Pleomorphic xanthoastrocytoma
Imaging Findings
Fig. 111.1: (A–C) Axial FLAIR showed a multifocal hyperintense lesion in the right frontal operculum, left superior frontal gyrus, and left middle frontal gyrus. Fig. 111.2: (A–C) Axial 3D-CISS showed a solid multifocal hyperintense lesion in the right frontal operculum, left superior frontal gyrus, and left middle frontal gyrus. Fig. 111.3: (A–C) Axial contrast-enhanced T1WI showed a solid, multifocal non-enhancement lesion in the right frontal operculum, left superior frontal gyrus, and left middle frontal gyrus. Fig. 111.4: T2 perfusion-DSC showed a low CBF in the large lesion on the right frontal operculum (cold perfusion).
Discussion
In the brain of a young patient with refractory epilepsy, intra-axial, cortical-based masses, with a cyst-like appearance, that lack perilesional edema or contrast enhancement demonstrate the typical imaging appearance suggestive of a multifocal dysembryoplastic neuroepithelial tumor (DNET).
Low-grade astrocytoma is also a T2-hyperintense, intra-axial mass that does not enhance; nevertheless, cortical involvement, the presence of a FLAIR hyperintense ring around the lesion, and scalloping of the overlying bone are not features of this entity. The most common appearance of gangliogliomas on MR imaging is that of a cyst, with a strongly enhancing mural nodule that frequently demonstrates some calcification in the lesion, which was absent in this patient.
Oligodendrogliomas typically manifest as a round or oval sharply marginated mass involving the cortex or subcortical white matter. Occasionally, the tumor margins are not well defined, as the tumor appears to blend imperceptibly into the normal adjacent brain parenchyma. Calcification, usually coarse in morphology, is noted in 20–91% of cases. Occasionally, cystic degeneration and hemorrhage may be seen. Subtle ill-defined enhancement following intravenous contrast material administration is seen in 15–20% of oligodendrogliomas and is associated with higher-grade tumors.
Angiocentric glioma typically presents as a cortical tumor with a hyperintense appearance on T1-weighted imaging and has a stalk-like extension of the lesion projecting to the ventricular surface, both of which were absent in this patient. Although usually superficial tumors, pleomorphic xanthoastrocytomas (PXAs) typically manifest as cystic tumors with a strongly enhancing mural nodule, often with an adjacent dural tail of enhancement, features not present in our case.
A benign and rare primary brain neoplasm, DNET is included in the neuronal and mixed neuronal-glial tumor category of WHO grade I. Although any lobe in the brain may be involved, DNET presents as a supratentorial and cortical intra-axial lesion that is characterized by a multinodular architecture and is usually located in the temporal lobe. Differentiating DNET from other brain tumors is important because patients with DNET benefit from complete resection, as the presence of residual tumor is a risk factor for relapse of seizures. Localized DNET is widely reported, but multifocal DNET remains an extremely rare entity, with only a handful of reported cases in the literature.
Clinicoradiologic criteria for the diagnosis of DNET are as follows: 1) a history of refractory partial seizures, with or without generalization, beginning before 20 years of age; 2) the absence of neurologic deficit; 3) the cortical location of the lesion; 4) the presence of remodeling of the inner table; and 5) the absence of mass effect and peritumoral edema.
A well-demarcated, lobulated, or multilobulated-appearing mass, DNET is typically hypodense on CT scan images, hypointense on T1, and hyperintense on T2-weighted MR images. It may demonstrate intratumoral cystic or microcystic changes in up to 40% of cases. Calcification on CT images can be seen in up to one-third of DNET tumors. Contrast enhancement can be seen in up to 40% of patients. On spectroscopy, it demonstrates increased myoinositol (mI) peak and is metabolically inactive on FDG and amino acid PET imaging.
Our patient’s clinicoradiologic presentation demonstrated all of the DNET diagnostic criteria. In addition, his imaging studies demonstrated other typical radiologic features of DNET, namely a wedge-like shape, the presence of internal septations, scalloping of the overlying cortical bone, a FLAIR hyperintense ring sign, high ADC values, and the absence of calcification and contrast enhancement, within his tumor.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


