CASE 114 Peter L. Munk and Anthony G. Ryan A 53-year-old man with bilateral ankle pain and a hard swelling overlying the anterior aspect of the left ankle came to our institution. Figure 114A Figure 114B Figure 114C A lateral plain film of the left ankle (Fig. 114A) shows a dense soft-tissue mass anterior to the tarsus in association with surface erosions of the talus and navicular. A corresponding CT of both feet (Fig. 114B) shows widespread hyperattenuating deposits within the soft tissues anterior to the tarsus on the left. A sagittal T1-weighted image of the left ankle (Fig. 114C) shows marked low signal intensity within the soft-tissue mass and also within the sinus tarsi (the normal high signal of sinus tarsi fat is absent). The cortical erosions are also demonstrated to good effect. Gouty tophus with erosions of underlying bones. The combination of findings on radiographs, CT, and MRI is essentially pathognomonic of tophaceous gout. Gout is a metabolic disease associated with increased serum uric acid levels (hyperuricemia) and attacks of acute, painful arthritis. Hyperuricemia by itself does not constitute gout. Typically, patients have had hyperuricemia for 10 to 12 years that is inadequately or not treated before the initial episode of gouty arthritis occurs. Gout is a metabolic disease associated with increased serum uric acid levels (hyperuricemia) and associated with intra- and periarticular deposition of monosodium urate crystals. Primary or idiopathic gout appears to be transmitted as an autosomal dominant process, with low penetrance in females. The vast majority of cases are idiopathic, although occasionally patients with inherited metabolic defects may develop gout, as might patients with malignancies producing marked nucleic acid turnover, such as leukemia. Caucasians appear to be more frequently afflicted than other racial groups, except for the Maori, where the prevalence among males reaches 10%. Urates are produced in the metabolism of purine nucleic acid, and either overproduction or under-secretion results in hyperuricemia. Symptoms occur with attacks of joint pain inflammation secondary to deposits of the urates in articular, periarticular, and tenosynovial soft tissues. Joints appear to be affected more than other tissues because of the lower solubility of urates in synovial fluid than plasma, and the lower temperature of peripheral joints further diminishes their solubility. The majority of these patients are middle-aged males. The most common site for an initial attack is the first metatarsophalangeal joint (podagra), although many other joints are commonly afflicted, such as the knee, elbow, wrist, and the small joints of the hands and feet. There is usually a sudden onset of severe pain centered on the joint that is associated with swelling, erythema, marked tenderness, and loss of function. The shoulder and spine are less frequently affected than most other sites.
Gout
Clinical Presentation

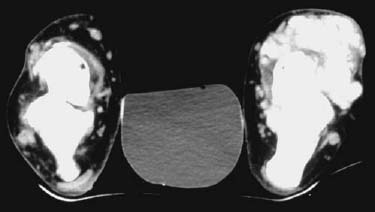

Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Etiology
Pathophysiology
Clinical Findings
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


