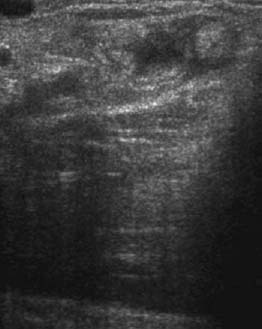
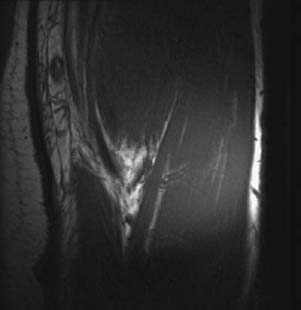
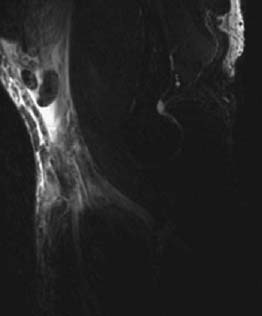
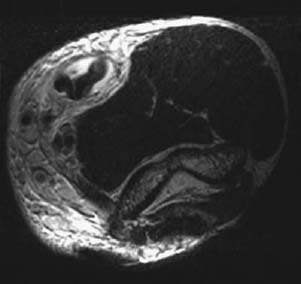
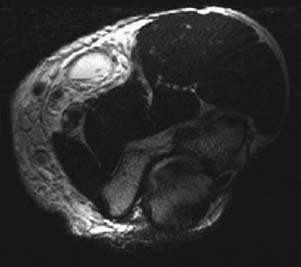
CASE 20 Anthony G. Ryan, Peter L. Munk, Laurel O. Marchinkow A 35-year-old male amateur bodybuilder presented with sudden pain in front of his elbow and a marked loss of power on elbow flexion. He claimed to have heard a pop and felt a tearing sensation while performing fast repeated biceps curls. On examination, there was obvious subcutaneous bruising and a visible mass just cephalad to the elbow joint that was accentuated on active flexion of the joint. The mass was tender, and elbow flexion against resistance was very painful. Figure 20A Figure 20B Figure 20C Figure 20D Sagittal linear ultrasound (Fig. 20A) of the painful lump mass demonstrates an irregular heterogeneous lesion consisting of multiple round/oval hyperechoic foci and a wavy, discontinuous fibrillar structure surrounded by anechoic material. A coronal T2-weighted image (Fig. 20B) shows marked high signal intensity and loss of definition in the expected position of the distal biceps tendon. The high signal intensity extends cephalad into the body of the biceps muscle. Discontinuous low signal intensity bands are visible within the heterogenous high signal. A sagittal T2-weighted fat-saturated image (Fig. 20C) at the same level shows two heterogeneous round/oval predominantly low signal intensity structures at the cephalad extent of a poorly marginated high signal intensity area. An axial T2-weighted image (Fig. 20D) at the level of the low signal intensity structures shows a wavy, nodular structure surrounded by high signal intensity that appears confined within an ovoid space configuration. An axial T2-weighted image (Fig. 20E) caudad to Fig. 20D shows the same ovoid space to be empty. Biceps tendon rupture. The ovoid high signal intensity collection is the empty tendon sheath at the level of the completely torn tendon. The wavy/nodular structures are the free ends of the tendon, retracted superiorly with muscle spasm and contraction. None—the appearances are pathognomonic. The long head of the biceps takes its origin from the supraglenoid tuberosity and inserts on the radial tuberosity, fanning out to form the bicipital aponeurosis attaching to the fascia of the forearm. It acts as a flexor of both the arm and the forearm. The two heads of the biceps join to form a common muscle belly, ending in a flattened, horizontally oriented distal tendon, typically measuring 7 cm in length. The distal biceps ruptures the dominant arm in 80% of cases and usually occurs in men. If no predisposing cause is identifiable, the typical age of rupture is 55. However, in bodybuilders or weight lifters, the injury occurs at a younger age, with abuse of anabolic steroids being a predisposing factor. In common with injuries at other tendon sites, tears usually occur secondary to acute trauma or overuse injury in athletes or, in the elderly and unconditioned, degenerative tendinopathy. The distal biceps tendon is covered by an extrasynovial paratenon, and the tendon is separated from the radial tuberosity by the radiobicipital bursa. Bursitis may accompany tendinosis and bicipital tear, the bursa enlarging as much as 5 cm when inflamed. The blood supply to the distal tendon is relatively poor 1 cm proximal to its insertion. This area, in addition, is prone to impingement between the radius and the ulna during pronation. The degenerated tendon is liable to become thickened, enlarged, and irregular with inflammation of the adjacent bursa. These factors will make further contributions to impingement likely, leading to further degeneration of the tendon. Bicipital tendinosis is relatively common (Figs. 20F, 20G
Distal Biceps Tendon Tear
Clinical Presentation
Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Etiology
Pathophysiology
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


