3 Arthrography
The articular spaces of the radiocarpal joint and the wrist are visualized with arthrography. Three-compartment arthrography is recommended to achieve a complete view. In the first session the midcarpal and the distal radioulnar joint are examined, and in the second session the radiocarpal joint is examined. Because of age-dependent degeneration of the ligaments and the triangular fibrocartilage complex (TFCC), the spectrum of arthographic variations is large. Conventional arthrography, which often correlates poorly with complaints, should therefore only be evaluated in the context of clinical findings. It is advantageous to combine arthrography and sectional imaging techniques in procedures termed MR arthrography or CT arthrography, both carrying the advantages of distension and optimal contrast of joint spaces with direct imaging of intra-articular soft tissues.
Anatomical Considerations
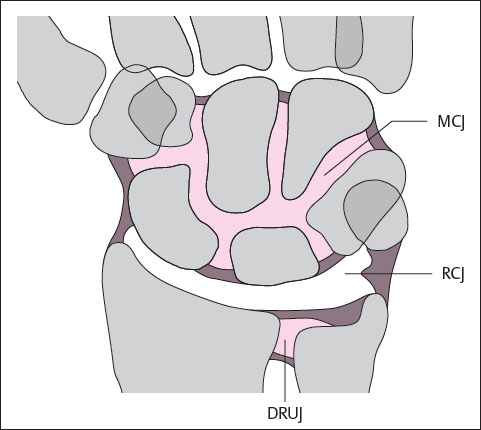
As demonstrated in Table 3.1 and Fig. 3.1 , the wrist consists of three large and numerous small synovial joint spaces (compartments).
Normally, there is no communication among the three large articular spaces, whereas intercompartmental communication among smaller joint spaces sometimes occurs as a variation of normal anatomy.
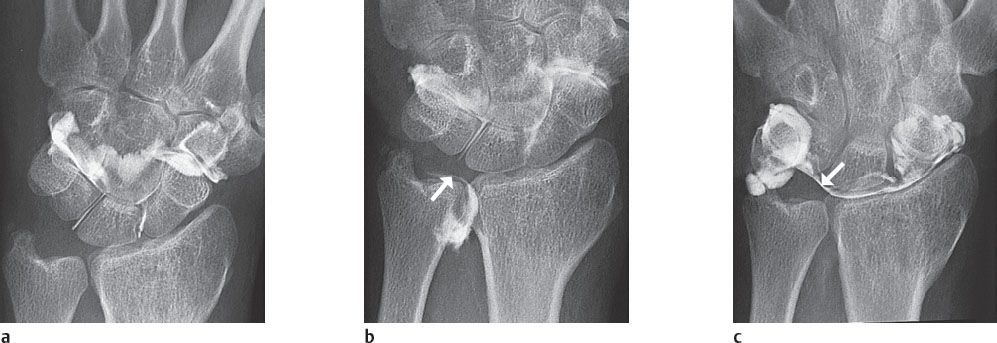
The midcarpal joint compartment (Fig. 3.2a) extends between the proximal and distal carpal row and often communicates with the carpometacarpal and intermetacarpal joint spaces of phalanges II–IV.
The distal radioulnar joint compartment (Fig. 3.2b) is bounded by the proximal surface of the triangular fibrocartilage complex and extends to a variable degree proximally.
The radiocarpal joint compartment in between (Fig. 3.2c) is bounded proximally by the articular cartilage of the distal radial section and the triangular fibrocartilage complex (TFCC). The distal boundary is the proximal carpal row and interosseous ligaments (scapholunate and lunotriquetral ligaments). In arthrography, the radiocarpal compartment has a C-shaped configuration with three recesses ( Table 3.2 ).
Large joint spaces
|
Small joint spaces
|
Finger joints
|
Arthrography of the Large Joint Spaces
Examination Technique
Arthrography is performed in the prone position with the patient’s arms stretched above his or her head and the wrist in pronation. After application of local anesthesia, a 25G cannula is inserted into the appropriate joint cavity under sterile conditions and fluoroscopic control, and digital or analog imaging with 1 image per second are carried out.
In conventional and CT arthrography, a mixture of two parts water-soluble contrast medium and one part local anesthetic is injected. This mixture is injected under continuous fluoroscopic control until the patient reports feeling pressure. The diagnostic advantage of adding local anesthetic to the mixture is that a reduction in pain (pain testing) indicates a probable cause of wrist complaints in this compartment.
In MR arthrography, a gadolinium solution is added to the above mixture to produce a solution with a ratio of 200:1 x-ray contrast medium/local anesthetic to gadolinium contrast medium.
All arthrographic accesses are on the dorsal side; the puncture site should always be chosen some distance from the reported painful area ( Table 3.3 ). This is the only way to avoid confusing a capsule defect caused by puncture trauma with a pathologic condition. The following peculiarities must be mentioned:
In midcarpal arthrography with radial access, the puncture site must be as far distal as possible, because otherwise the radiocarpal compartment can be filled with contrast medium via its scaphoid recess, which extends far in a distal-dorsal direction. A volume of 1–2 ml of contrast medium is generally sufficient.
Due to the physiological inclination of the radial joint surface 10° in the palmar direction, it is advantageous to project the radiocarpal joint by tilting the x-ray tube in a superior-inferior direction. The same effect can be achieved with a positioning wedge under the wrist. Puncture of the tabatière (“snuff box”) should be avoided because the dorsal branch of the radial artery can be found here. Puncture between the scaphoid and the lunate bone should also be avoided, since the midcarpal compartment can be filled with contrast medium if a deep recess is present. A volume of 2–3 ml of the contrast mixture is injected.
The distal radioulnar joint can hold about 1ml of contrast medium.
|
Multicompartment Arthrography
Incomplete (noncommunicating) defects can, under certain conditions, escape detection in single-compartment arthrography. For example, avulsion of the triangular fibrocartilage complex from its proximal ulnar attachment on the styloid process will not be seen if the arthrographic examination is limited to the radiocarpal joint. For this reason, the arthrographic examination should include all three large compartments. With nonspecific complaints concerning the wrist, only visualization of all articular spaces can reveal communicating and noncommunicating defects. Performance of three-compartment arthrography is therefore justified, particularly since defects can be present in several compartments.
The suitable injection sequence for this examination is shown in Table 3.4 . This procedure offers the advantage of showing all joint compartments without overlapping, since the contrast medium injected in the first session is absorbed during the two-hour interval. By applying the digital subtraction technique during the injection, all compartments can be examined in immediate succession. However, arthrographic stress films cannot be acquired with the subtraction method.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


