33 Osteopathies Caused by Hormones, Vitamins, Medications, or Toxins
A number of diseases caused by disorders in hormone or vitamin metabolism, side effects of medication, or toxins also affect the skeleton and soft tissues. The clinical manifestations are often displayed earlier in the hand than in other skeletal locations. The structural lesions are detectable even insurvey radiographs.
Endocrine Osteopathies
Acromegaly
Pathoanatomy and Clinical Symptoms
Hypersecretion of growth hormone (STH) from the adenohypophysis leads to excessive growth of the peripheral skeleton. The physiognomy is characterized byenlargement and coarsening of the skull, the lower jaw, the ears, the nose, the tongue, and the hands (pawlike hands) together with a general enlargement of the internal organs (splanchomegaly).
Diagnostic Imaging
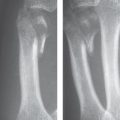
The main signs are excessive bone growth with osteopenia and fibro-ostoses, as well as thickened soft tissues ( Table 33.1 , Fig. 33.1 ).
The cause of the cone-shaped/bell-shaped epiphyses is a disturbance in enchondral ossification. Epiphyseal growth is blocked, whereas metaphyseal growth continues undisturbed.
Hypopituitarism
Pathoanatomy and Clinical Symptoms
There is either a complete (Simmond disease) or partial insufficiency of the adenohypophysis, with decreased serum levels of STH, corticoids, and thyroid and gonadal hormones. Adynamia, an expressionless, pale face, secondary amenorrhea, and atrophy of the genital organs are among the many clinical symptoms.
Diagnostic Imaging
The findings are summarized in Table 33.2 and Figure 33.2. The index for the thickness of the cortical bone is measured at the narrowest part of the second and third metacarpals (Barnett—Nordin’s index, see Figure 31.2 ).


Adrenogenital syndrome (AGS)
Pathoanatomy and Clinical Symptoms
There is a disturbance in the synthesis of corticosteroids in the adrenal cortices. The congenital form (hydroxylase deficiency) must be differentiated from the acquired form (benign or malignant adrenal tumors). In the congenital form, a decreased corticoid concentration in the serum reactively leads to increased production of androgenous hormones via the adrenocorticotropic hormone (ACTH). In early childhood, this leads to isosexual or heterosexual virilization and later to pseudopubertas praecox. Special forms of AGS are associated with electrolyte depletion or hypertonia.
|
Diagnostic Imaging
There is increased growth in length up to primary-school age, and a distinct acceleration of bone age may be found radiographically up to the age of 12 or 13 years. This is followed by accelerated closure of the growth plates. Children who were formerly exceptionally tall then fall behind in growth in comparison to their age group.
Hyperparathyroidism
The forms of hyperparathyroidism are discussed in Chapter 31.
Hypoparathyroidism
Pathoanatomy and Clinical Symptoms
Primary idiopathic hypoparathyroidism is rare and may have a familial occurrence or may be related to pluriglandular syndromes or autoimmune endocrinopathies. Parathyroid hormone deficiency most commonly occurs as secondary hypoparathyroidism after excision or lesions to the parathyroid glands during surgery of thyroid and larynx or after radiotherapy of the thyroid gland. Parathyroid hormone deficiency leads to decelerated bone remodeling, hypocalcemia, and neuromuscular dysfunction.
Diagnostic Imaging
Long-term hypoparathyroidism results in generalized or food hyperostosis of cortical and cancellous bone, as well as soft-tissue calcification. In the hand, these changes show only a mild expression. Occasionally enthesiopathies (Chapter 28), tendon/ligament calcification, and premature closure of the epiphyseal plates in children have been observed.
Pseudohypoparathyroidism and Pseudo-pseudohypoparathyroidism
Pathoanatomy and Clinical Symptoms
Both diseases are caused by a genetic deficiency of the phosphate-transmitting enzyme, adenylate cyclase. This leads to an end-organ resistance to parathyroid hormone in the bones and kidneys. The serum level of parathyroid hormone is elevated. In pseudohypoparathyroidism (PHP) there is hyperphosphatemia with reactive hypocalcemia, whereas in pseudo-pseudohypoparathyroidism (PPHP) the serum phosphate and calcium levels are normal. The clinical appearance of PHP and PPHP is characterized by short stature, rounded face, and brachydactyly.
Diagnostic Imaging
The radiographic manifestations of PHP and PPHP are identical. In the hand, primary signs are premature fusion of growth plates and shortening of all metacarpals (especially the thumb, index, and little fingers), and broad and short phalanges with pseudoepiphyses ( Fig. 33.3 ). Small, broad-based exostoses can appear on the phalangeal diaphyses. Soft-tissue calcifications are usually symmetrical and plaque-shaped in subcutaneous tissue. Small soft-tissue ossifications can be found in para-articular location.
Hypothyroidism
Pathoanatomy and Clinical Symptoms
Causes of childhood hypothyroidism (“cretinism”) can be aplasia or dysplasia of the thyroid gland, an exogenous iodine deficiency, or disturbed metabolism of iodine. Clinical symptoms include disproportional dwarfism, the characteristic facial physiognomy, hearing loss, and lowered intellectual maturity.
Diagnostic Imaging
The criteria in Table 33.3 and Fig. 33.4 depend on the onset and duration of the thyroid deficiency. Delayed bony maturation can be compensated with hormone substitution, but skeletal abnormalities due to bone dysgenesis persist.
In adult hypothyroidism, bone abnormalities are mild and frequently include osteoporosis with thinning of the compact bone. If hypothyroidism was alreadypresent in childhood, residual findings of childhood hypothyroidism as listed in Table 33.3 may be observed ( Fig. 33.5 ).
|



Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


