Pneumonias are usually classified according to the infecting organism because the cause dictates the treatment. However, imaging is usually poor at predicting even the broad category of infectious agent, let alone the specific organism. 1 Furthermore, preexisting lung disease, particularly emphysema, can modify the appearance of pulmonary consolidation. Nevertheless, imaging has many important roles in patients with suspected pulmonary infection. The chest radiograph is the primary method of establishing the presence of pneumonia and of determining its location and extent. Predisposing conditions, for example bronchial carcinoma, may be visible, and complications, such as pleural effusion, empyema, and abscess formation, are readily demonstrated. Chest radiography is also a satisfactory method of following the response to treatment. In complicated cases, particularly immunocompromised patients, 2 or in patients in whom response to treatment is unexpectedly slow, computed tomography (CT) has a role. 3
The essential radiographic feature of pneumonia is pulmonary consolidation, which may show cavitation and may be accompanied by pleural effusion. The appearance varies almost infinitely from one or more small, ill-defined shadows to large airspace shadows involving the whole of one or more lobes. The pattern depends to some extent on the infecting organism, and on the integrity of the host’s defenses (see below).
Pneumonias are sometimes divided according to their chest radiographic appearances into bronchopneumonia, lobar pneumonia, spherical (round or nodular) pneumonia, and interstitial pneumonia (Box 5.1). Although widely used, these terms have limited value because the same organism may produce several patterns and because patterns often overlap in an individual patient.
• Bronchopneumonia: airways involved with filling of adjacent acini giving a nodular pattern and patchy consolidation; associated volume loss. May reflect overspill of infected secretions from tuberculous or bacterial abscess cavity
• Lobar pneumonia: homogeneous consolidation bounded by fissures, with or without air bronchogram. No volume loss. Commonest manifestation of community-acquired pneumonia
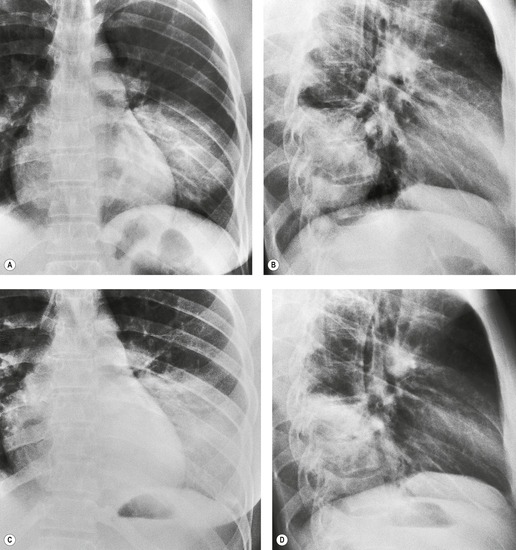
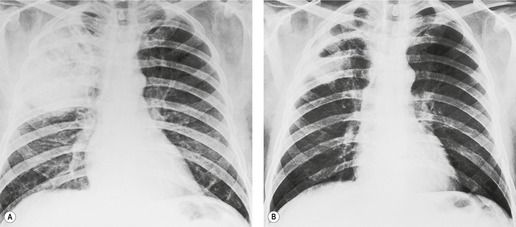
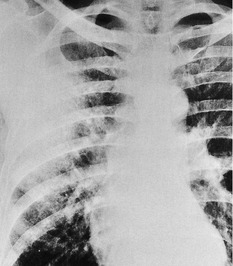
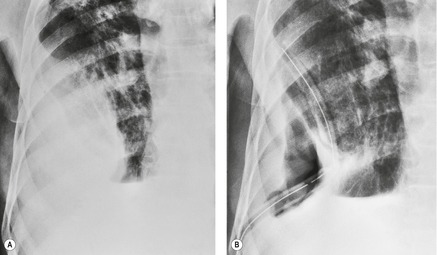
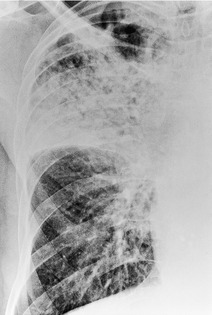
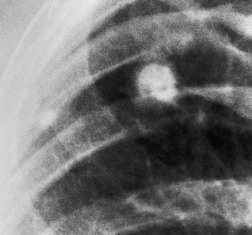
• Spherical (round): ill-defined round area of consolidation, with or without air bronchogram. Most frequent in childhood. May progress to lobar pneumonia
• Interstitial pneumonia: widespread peribronchial thickening and interstitial shadowing. Often associated with areas of subsegmental collapse. M. pneumoniae or viral infections commonest causes
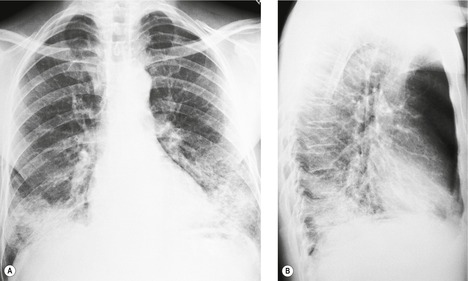
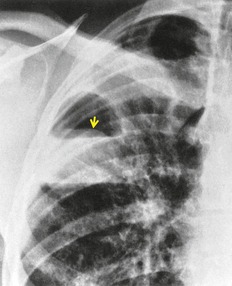
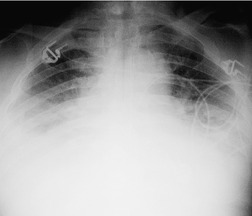
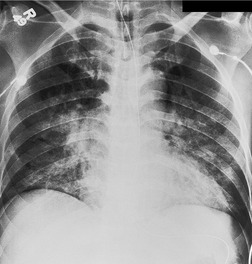
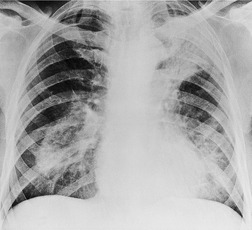
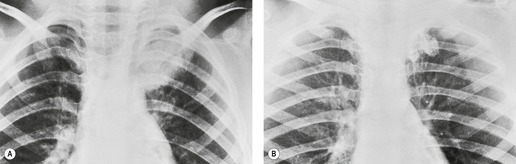
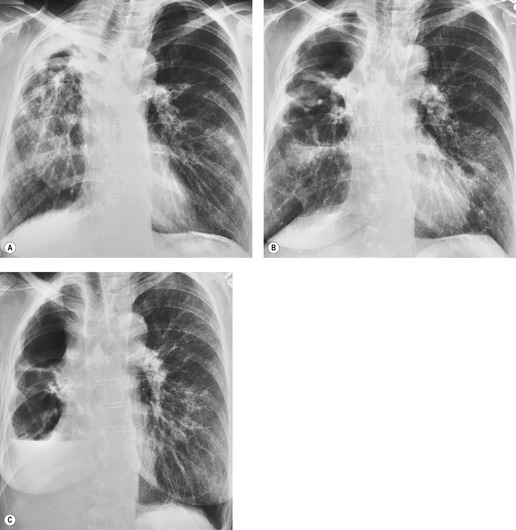
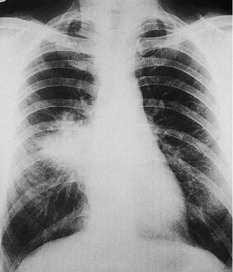
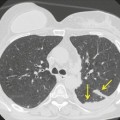
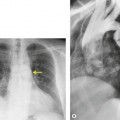
In bronchopneumonia the inflammatory exudate is multifocal and centered on large inflamed airways, involving some acini and sparing others. On the chest radiograph, bronchopneumonia is characterized by patchy consolidation, loss of volume, and absence of air bronchograms (Fig. 5.1). When affected areas coalesce, the shadowing may become more uniform and resemble lobar pneumonia. Although the term ‘segmental consolidation’ is in common use, consolidation conforming precisely to segmental anatomy is, in fact, extremely rare.
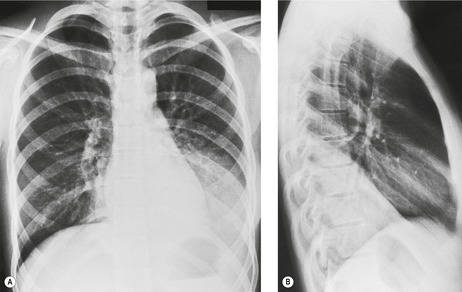
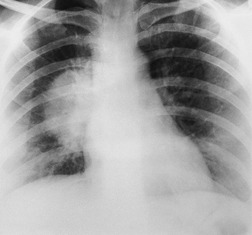
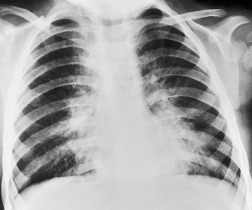
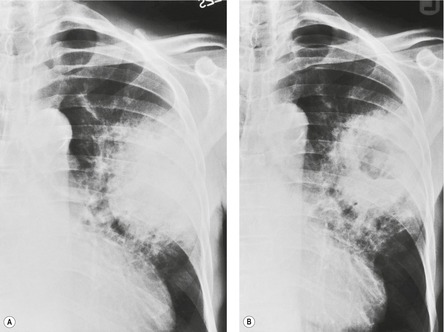
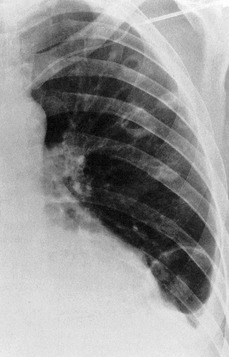
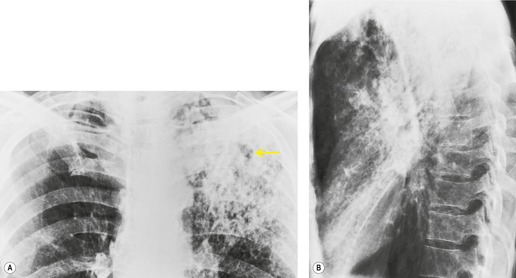
In lobar pneumonia (Fig. 5.2) the inflammatory exudate begins in the distal airspaces and spreads across segmental boundaries, giving rise to homogeneous and widespread consolidation. Eventually the pneumonia may involve a whole lobe, but usually symptoms develop before the entire lobe is consolidated and then antibiotic therapy halts the process. The consolidation is usually confined to one lobe, although multilobar involvement is not uncommon. Because the airways are not primarily affected, there is little or no volume loss and visible air bronchograms are common.
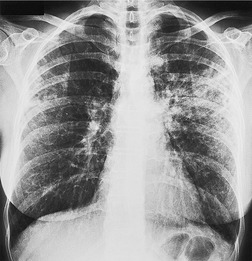
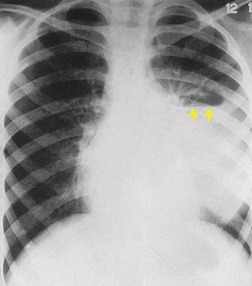
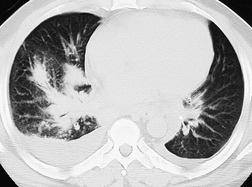
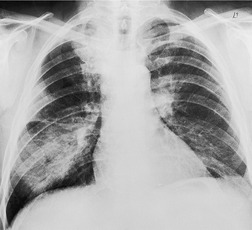
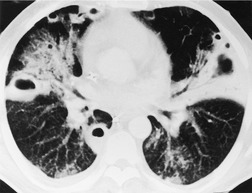
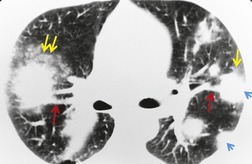
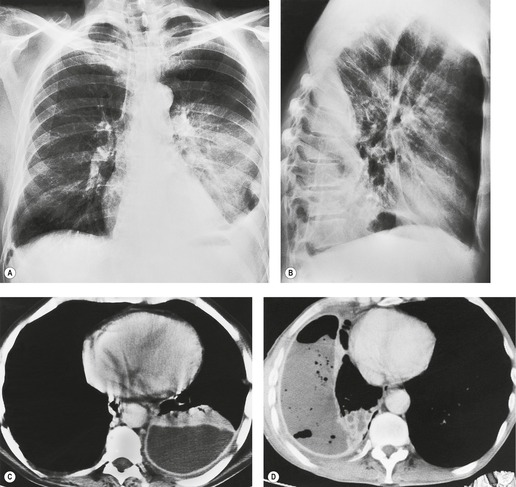
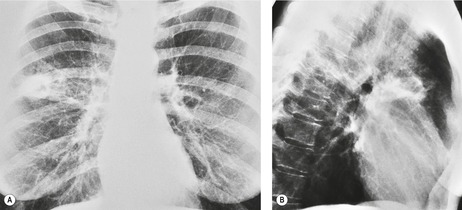
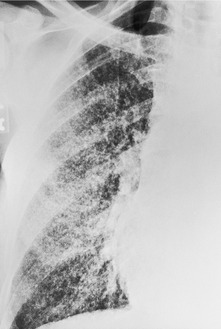
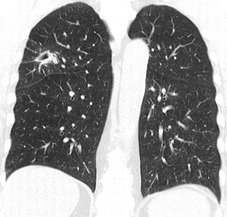
Interstitial pneumonia refers to a radiographic pattern comprising extensive peribronchial thickening and ill-defined reticulonodular shadowing of the lungs, which may be relatively localized or may be widespread (Fig. 5.4). Associated patchy subsegmental or discoid atelectasis is common. This pattern, although it may show a lobar or segmental distribution, is frequently independent of the lobar architecture of the lung. The usual causes are viral and Mycoplasma pneumoniae infections.
The chest radiograph is the most commonly ordered imaging investigation in patients with suspected pneumonia; even so, the majority of individuals with a community-acquired pneumonia are diagnosed on clinical grounds alone, without recourse to chest radiography. Although not well documented, it seems likely that radiographic abnormalities become apparent within 12 hours after the onset of symptoms of (bacterial) pneumonia. 4 CT may be helpful in individuals in whom there is a strong clinical suspicion of pneumonia but a normal or near normal chest radiograph. 5 CT is also useful in patients with a suspected complication (for example, empyema) or underlying cause (for example, bronchial obstruction) and CT may occasionally help to refine the differential diagnosis of the causative organism,3.5.6. and 7. although in general there are few CT features that discriminate between bacterial pneumonias.3. and 8.
DIAGNOSING THE CAUSE OF PNEUMONIA
Some pneumonias caused by viruses or M. pneumoniae are self-limiting and resolve without treatment, whereas bacterial pneumonias require accurate diagnosis and therapy if serious complications, and even death, are to be avoided. The choice of which antibiotic to use may have to rest on a combination of clinical findings, radiographic features, and an initial Gram stain of the sputum9 because the results of bacteriologic tests may be delayed and are sometimes uninformative. 10 Many empirical factors aid the decision-making in managing patients with pneumonia:
• The age of the patient and any history of exposure to a specific organism. In infants viral infections are the dominant cause of pneumonia, and Mycoplasma infection is an important cause in young children. 11 Bacterial pneumonia is relatively rare at an early age. In adults with radiographically evident pulmonary consolidation the commonest cause is bacterial infection.
• The source of the infection, particularly whether it was acquired in the hospital or in the community. Pneumococcal, chlamydial, mycoplasmal, and viral pneumonias are the commonest community-acquired pneumonias in adults.12. and 13.Staphylococcus aureus, Streptococcus pyogenes, Klebsiella, Rickettsia, and Legionella pneumophila are less frequent agents. By contrast, Gram-negative bacilli, S. aureus, anaerobic organisms, and pneumococci are particularly prevalent causes in hospital-acquired infections.14. and 15. Nearly half the cases of hospital-acquired pneumonia have more than one pathogen. 14
• The character of the illness. Bacterial pneumonia typically presents as an acute illness with chest pain, chills, high fever, and cough productive of purulent sputum. Neutrophilia is common. Mycoplasma and viral pneumonias, on the other hand, usually have prodromal symptoms, mild pyrexia, and less sputum; neutrophilia is absent and the white blood cell count is usually only slightly elevated.
• Predisposing conditions. The list of predisposing conditions is long and complex. For example, aspiration pneumonia, which is most often due to anaerobic organisms, Gram-negative bacteria, or S. aureus, is particularly prevalent in patients who have a history of alcohol misuse, have had recent general anesthesia or a bout of unconsciousness, or have disturbances of swallowing. 16 Pneumococcal pneumonia is particularly likely in sickle cell disease and following splenectomy. Pseudomonas aeruginosa or S. aureus is the likely pathogen responsible for pneumonia in patients with cystic fibrosis.17. and 18. Patients with chronic obstructive pulmonary disease are more prone to exacerbations caused by Haemophilus influenzae and Branhamella catarrhalis.19 Patients who are immunocompromised present a special category and are discussed in Chapter 6.
Before considering individual pneumonias, it may be helpful to point out a few generalizations regarding pulmonary infection of the immunocompetent host:
• Consolidation of all or most of a lobe is usually bacterial in origin (see Fig. 5.2), and postobstructive pneumonia should be strongly considered, particularly in patients who may have carcinoma of the bronchus. When lobar consolidation is due to a primary bacterial infection, the usual organism is Streptococcus pneumoniae (pneumococcus). Occasionally the infection is due to Klebsiella, S. aureus, Mycobacterium tuberculosis, or L. pneumophila or to aspiration of anaerobic or Gram-negative bacteria from the upper respiratory tract or pharynx. Expansion of the lobe is a famous (but unreliable) sign that is said to suggest pneumococcal or Klebsiella pneumonia.
• Aspiration pneumonia frequently causes patchy consolidation in the dependent portions of the lungs (see Fig. 5.1). Consolidation is usually multilobar and bilateral in distribution, but the patterns of aspiration pneumonia are probably more variable than generally thought.
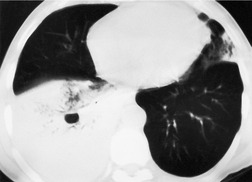
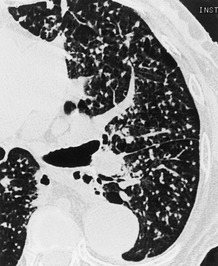
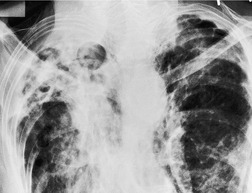
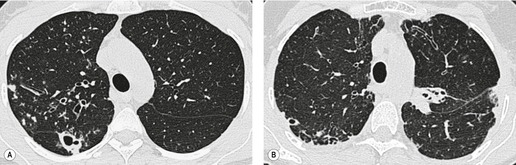
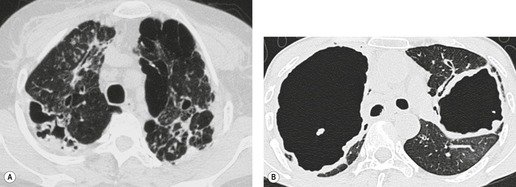
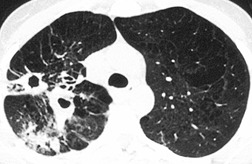
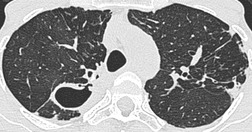
• Consolidation with cavitation (Fig. 5.5) suggests bacterial or fungal disease rather than viral or Mycoplasma infection. The bacteria that commonly cause cavitation are S. aureus, Gram-negative bacteria (especially Klebsiella, Proteus, and Pseudomonas), anaerobic bacteria, (particularly in patients with poor oral hygiene) and M. tuberculosis. A large solitary abscess in a patient without underlying lung disease is usually due to anaerobic bacteria. Such abscesses are usually due to aspiration of oropharyngeal secretions, alone or in combination with impairment of local or systemic host defense mechanisms. 20 Pneumatocele formation can be difficult to distinguish from cavitation (Fig. 5.6). When pneumatoceles are due to pneumonia, the responsible organism is often S. aureus, although pneumatoceles have been described in other infections, including Pneumocystis jirovecii. Care needs to be taken to avoid misdiagnosing cavitation or pneumatocele formation when there are focal transradiancies within consolidation due to underlying emphysema. Emphysematous bullae within the consolidated lung readily resemble cavitation. 21 Pulmonary gangrene is a rare but interesting form of cavitation that produces sloughed lung within a large cavity secondary to thrombosis or involvement of the pulmonary vessels as they pass through the pneumonia (Fig. 5.7). 22S. pneumoniae and Klebsiella23. and 24. are the most common bacteria responsible for this phenomenon. Pulmonary gangrene has also been described with M. tuberculosis, 23 possibly with anaerobic bacteria, 24 with invasive Aspergillus infection, and with mucormycosis particularly in the immunocompromised host. 25
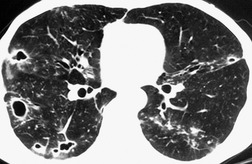
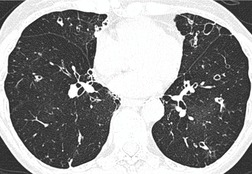
• Pneumonia that presents with focal or widespread, small, ill-defined reticulonodular shadows (Fig. 5.8), whether or not lobar or segmental consolidation is also present, is likely to be due to viral or mycoplasmal infection.30. and 31. In exceptional cases fungal and streptococcal infection gives rise to this pattern.
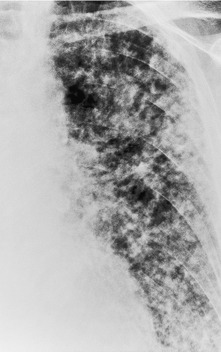
• A miliary nodular pattern in the lungs has many causes. When it is due to infection, the likely organisms are M. tuberculosis (Fig. 5.9) and various fungi. The nodules are even in size, usually 2–4 mm in diameter, well defined, and uniformly distributed.
• Patchy upper lobe consolidation (Fig. 5.10) is very suggestive of tuberculous or fungal infection, notably histoplasmosis but occasionally North American blastomycosis, cryptococcosis, and coccidioidomycosis. Patchy lower lobe consolidation together with volume loss is suggestive of aspiration pneumonia.
• Large pleural effusions are most commonly associated with pneumonia caused by anaerobic bacteria, Gram-negative bacteria, S. aureus, or S. pyogenes. Empyemas are radiographically indistinguishable from uninfected pleural effusions, but empyema should be considered if the effusion is large, delayed in appearance, or loculated, particularly if it loculates rapidly.
• The majority of pneumonias resolve radiographically within a month, often within 10–21 days, and most of the remainder by 2 months. The most indolent pneumonias are those caused by tuberculosis, anaerobes, Coxiella burnetti, Legionella pneumophila, or Chlamydia psittaci and with some cases of M. pneumoniae pneumonia. Consolidation persisting beyond 2 months represents delayed resolution, and an explanation should be sought. The most likely reasons are that the patient is old or debilitated and not fully immunocompetent. Alternatively, the pneumonia may have been extensive or have been complicated by atelectasis or cavitation. If none of these explanations appears satisfactory, a predisposing local cause such as obstructing neoplasm should be actively excluded. 32
• Diagnosing pneumonia in ventilated or postoperative patients can be very difficult. Portable chest radiography may not disclose basal consolidation in approximately a quarter of patients following abdominal surgery. 33 Pneumonia, edema, acute respiratory distress syndrome (ARDS), infarction, and hemorrhage have overlapping signs, so that a confident diagnosis based on radiographic features alone is often impossible.34.35. and 36. In patients with ARDS, CT may reveal areas of cavitation or empyema not shown on chest radiography that are suggestive of coexisting infection. 37 CT appearances are reasonably good at distinguishing between ARDS patients with and without ventilator-associated pneumonia, although no single CT feature is discriminatory. 38
• The distinction between normality and early community-acquired pneumonia is often difficult and has poor interobserver agreement. 39
BACTERIAL PNEUMONIA
Streptococcus pneumoniae pneumonia
S. pneumoniae (pneumococcal) pneumonia occurs at any age, is the most common community-acquired bacterial pneumonia,13. and 40. and is the most frequent (approximately 40%) type of pneumonia that results in hospitalization. 41 Dementia, seizure disorders, institutionalization, smoking, previous splenectomy, congestive heart failure, and various chronic illnesses, including human immunodeficiency virus (HIV) infection, are all predisposing factors. 42 Given a mortality rate of up to 25% of susceptible individuals, polyvalent polysaccharide pneumococcal vaccination is recommended for at-risk elderly and very young individuals. 43 The initial symptoms of pneumococcal pneumonia typically include sudden onset of high fever, pleuritic pain, and cough productive of sputum that is sometimes streaked with blood.
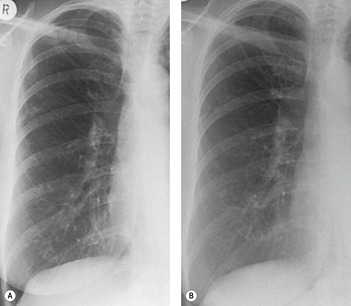
A variety of radiographic patterns are described (Box 5.2). Pneumococcal pneumonia is the prototype pathologic condition for lobar consolidation (Figs 5.2 and 5.11). Bacteria are inhaled into the periphery of a lobe where they incite an intense inflammatory reaction, which is seen radiographically as an area of nonsegmental shadowing (Fig. 5.12). Air bronchograms may be evident. The exudate spreads rapidly across interalveolar connections rather than via the bronchial tree. It crosses segmental boundaries through the pores of Kohn and therefore does not show a segmental pattern. If untreated the pneumonia may involve the whole of the lobe, which may be expanded by the intense exudate. Frequently the gravitationally dependent portions of the lobes are the most densely opacified. Sometimes more than one lobe is involved. Early in its course, before any pleural boundaries have been reached, the pneumonia may be spherical (Figs 5.3 and 5.13), a phenomenon seen most frequently in children.
Some reports have emphasized that the more usual pattern is patchy or peribronchial consolidation (Fig. 5.14), patterns that occurred in 57 (61%) of 94 patients described by Ort et al. 44 and in 28 (70%) of 40 patients in Kantor’s series. 45 However, lobar consolidation is overall the most frequent (67% in the series of Levy et al.). 9 A widespread, small nodular and linear pattern resembling interstitial disease is seen in 13–22% of patients;9. and 45. others do not emphasize this pattern, presumably regarding it as one of the bronchopneumonic varieties. Another series has emphasized that lobar consolidation remains the most frequent radiographic pattern and, interestingly, this was unaffected by HIV seropostivity. 46 With appropriate treatment the pneumonia usually clears within 14 days. Enlarged lymph nodes, in the drainage path, are a frequent (approximately 50%) accompaniment. 47 A study that compared the CT findings of Chlamydia pneumoniae, Mycoplasma pneumoniae and S. pneumoniae concluded that there were numerous common features but that nodular bronchovascular thickening and airway dilatation were more frequent in C. pneumoniae.48
Pleural effusion is seen in up to half of patients49 and occasionally, particularly if treatment has been delayed, the effusion turns into an empyema. The presence of parapneumonic effusions correlates with the duration of symptoms before admission, with bacteremia, and with prolonged fever after commencement of therapy. 50 Cavitation is distinctly unusual (Fig. 5.15), 42 and when it occurs may be caused by an accompanying anaerobic infection. A very rare complication is pulmonary gangrene. 24 Ipsilateral lymphadenopathy is frequently (54%) identifiable on CT in patients with pneumococcal pneumonia. 47
S. pyogenes and other types of streptococcus cause pneumonia much less frequently than S. pneumoniae. In the early part of last century S. pyogenes was a major cause of pneumonia in both adults and children. Although comparatively rare it remains an important and potentially fatal pneumonia.51. and 52. It may complicate viral infections or may follow streptococcal upper respiratory tract infections. On chest radiographs, S. pyogenes pneumonia appears as lower lobe-predominant, confluent, or patchy consolidation. Large pleural effusions and empyema are common. 53
Staphylococcal pneumonia
S. aureus is a relatively uncommon cause of community-acquired pneumonia, but in many hospitals it is becoming a particular problem because of the development of methicillin-resistant strains, particularly for patients in intensive care units. 54 There is up to a 20-fold increased mortality risk for patients with pneumonia caused by methicillin-resistant S. aureus (MRSA), compared with those with nonresistant S. aureus pneumonia.55. and 56. In the community, infants and elderly individuals (particularly those with influenza) are particularly susceptible. Pneumonia caused by hematogenous spread may result from endocarditis, thrombophlebitis, or staphylococcal infection of indwelling catheters. Septicemic infection is also seen in drug addicts and immunocompromised patients.
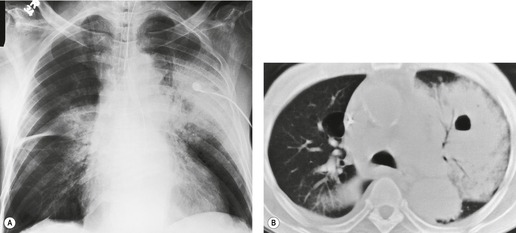
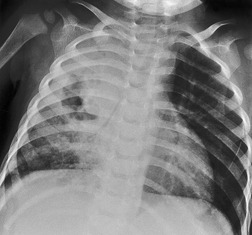
Typically the plain chest radiograph (Fig. 5.16) shows patchy segmental consolidation, or a more nodular bronchopneumonic pattern, often with loss of volume. On CT a tree-in-bud pattern and centrilobular nodules may be present. 8 The consolidation may spread rapidly and become confluent, resembling lobar pneumonia (Fig. 5.17). Several lobes are usually involved, 57 and the disease may be bilateral. There do not appear to be any differences between the radiographic pattern of MRSA and that of non-MRSA infection. 58 Abscess cavities may form within the pneumonia and are common at any age (see Fig. 5.17). Pneumatoceles (Fig. 5.18) are more common in childhood than adult infection57 and may lead to pneumothorax. Pleural effusions, which may develop rapidly, are common. Empyema formation is a frequent and serious complication, particularly in children. Septicemic staphylococcal infection, in contrast with infection following aspiration, causes multiple spherical (round) consolidations (bloodborne septic emboli), which may cavitate (Box 5.3). 59
• Patchy or bronchopneumonic consolidation – unilateral or bilateral
• Acinar nodules (up to 1 cm diameter) frequent
• Tree-in-bud and centrilobular nodules identifiable on CT
• Abscess formation within consolidation common
• Pneumatoceles more frequent in children than in adults
• Pneumothorax and pleural effusions (empyema) are common complications
Anthrax
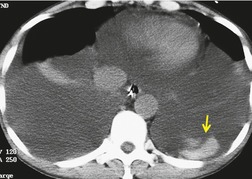
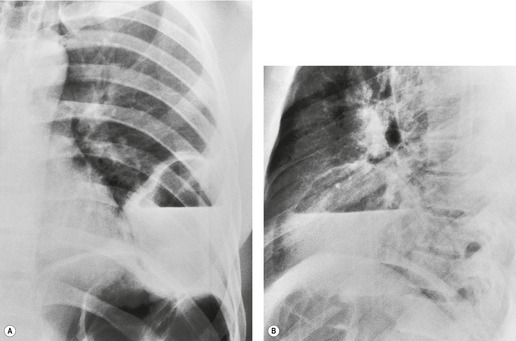
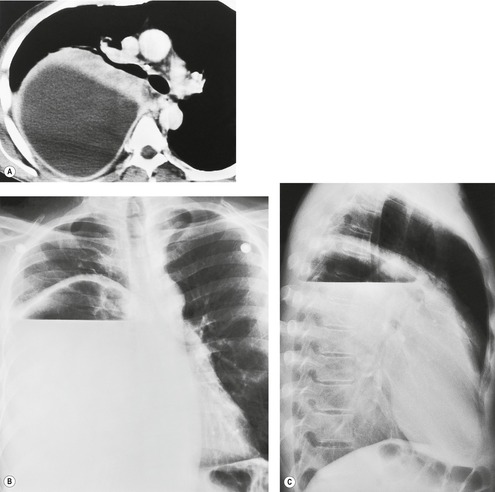
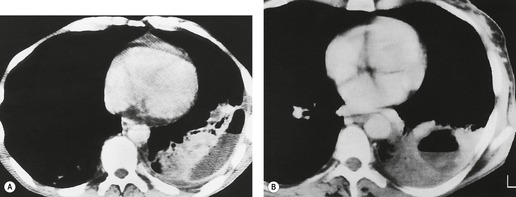
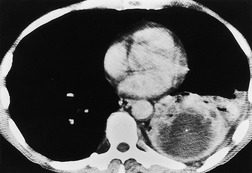
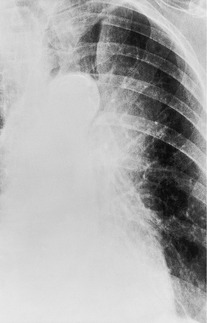
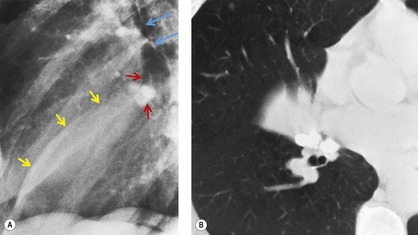
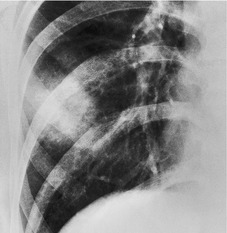
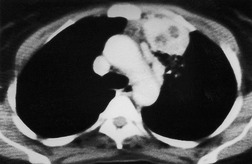
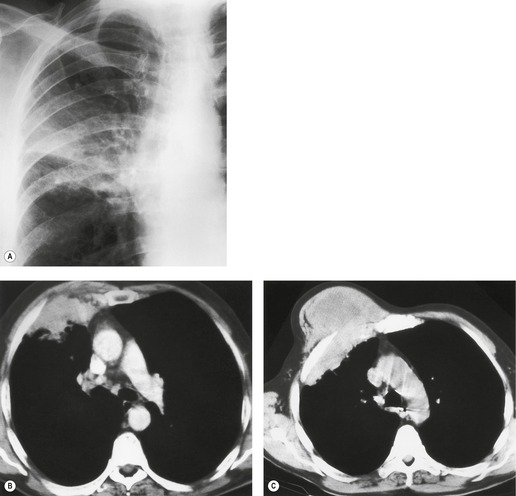
Anthrax is due to Bacillus anthracis, a Gram-positive aerobic bacillus. It is usually acquired from contact with infected goats or their products, particularly unfinished hides and wools imported from endemic areas in Asia, the Middle East, or Africa (Fig. 5.19). Indigenous anthrax is extremely rare in the USA and Europe but awareness of the disease increased sharply after use of the bacteria to spread infection by terrorists in 2001.60.61.62.63. and 64. The spores may be inhaled directly into the lungs, but cutaneous anthrax is the commonest clinical presentation. The spores are carried to regional lymph nodes, from which they may disseminate to the lungs and cause hemorrhagic pneumonia. Striking mediastinal widening, caused by lymphadenopathy, is a particularly common radiographic feature65. and 66. (Fig. 5.20). Chest radiography may also show patchy consolidation, particularly at the bases, and pleural effusions. The imaging of two survivors of anthrax inhalation is described in detail by Earls et al. 66 In neither case was the diagnosis of anthrax suggested on the basis of plain radiography; nevertheless, the authors emphasize the pathognomonic combination of a widened mediastinum in a previously fit individual with ‘flulike’ symptoms and known anthrax exposure. CT shows more extensive parenchymal and nodal involvement than plain radiography. The consolidation is often bronchocentric and perihilar (Fig. 5.21) and the enlarged lymph nodes may be of increased attenuation (on an unenhanced CT examination), presumably reflecting intranodal hemorrhage (Fig. 5.22). Similarly, hyperattenuating recent blood clot may be identifiable within pleural effusions (Fig. 5.23); the effusions may be persistent in survivors. 64 Following administration of intravenous contrast the enhancing rims of hemorrhagic lymph nodes may become visible, particularly on delayed scans. 67 Ancillary features on CT include mucosal thickening within the large airways, pericardial effusion and opacification of the mediastinal fat by hemorrhage and edema. 67
(With permission from Earls JP, Cerva D Jr, Berman E, et al. Inhalational anthrax after bioterrorism exposure: spectrum of imaging findings in two surviving patients. Radiology 2002;222:305–312. Copyright Radiological Society of North America.)
(With permission from Earls JP, Cerva D Jr, Berman E, et al. Inhalational anthrax after bioterrorism exposure: spectrum of imaging findings in two surviving patients. Radiology 2002;222:305–312. Copyright Radiological Society of North America.)
(From Mayer T, Bersoff-Matcha S, Murphy C, et al. Inhalational anthrax: clinical presentation of two cases following bioterrorism exposure. JAMA 2001;286:2549–2553. Copyright American Medical Association. All rights reserved.)
(With permission from Earls JP, Cerva D Jr, Berman E, et al. Inhalational anthrax after bioterrorism exposure: spectrum of imaging findings in two surviving patients. Radiology 2002;222:305–312. Copyright Radiological Society of North America.)
Gram-negative bacterial pneumonia
Many aerobic Gram-negative bacteria cause pneumonia. 68 The incidence of Gram-negative bacterial pneumonia has risen from less than 10% in the 1960s to approximately 20%, and these bacteria are responsible for the majority of nosocomial pneumonias. 15 The most important are Enterobacteriaceae (notably Klebsiella, Enterobacter, Serratia marcescens, Escherichia coli, and Proteus mirabilis), P. aeruginosa, Acinetobacter, Haemophilus influenzae, and L. pneumophila. Together with S. aureus these organisms are a major cause of morbidity and mortality in hospital patients.15.37. and 69. These bacteria contaminate hospital equipment such as ventilators and the soaps, liquids, or jellies used in the care of wounds and catheters. The radiographic pattern of the Gram-negative bacterial pneumonias is generally nonspecific70.71.72.73. and 74. and ranges from small ill-defined nodules to patchy consolidation (Fig. 5.24), which may sometimes be confluent and resemble lobar pneumonia or even pulmonary edema. 75 Cavitation in Gram-negative pneumonia is common (Fig. 5.25), 76 but radiographic lucencies in areas of consolidation, although often caused by abscess formation, are sometimes due to spared normal acini and lobules surrounded by pneumonia. 72
P. aeruginosa is a common nosocomial pathogen; it has a propensity for colonizing bronchiectatic airways, particularly in patients with cystic fibrosis. 77 It only occasionally causes community-acquired pneumonia in otherwise healthy individuals. 78 Patients with bronchiectasis who are colonized with P. aeruginosa tend to have more severe bronchiectasis, in terms of functional deficit79 and morphologic abnormalities on CT, 80 than noncolonized individuals; whether this reflects the deleterious effects of P. aeruginosa infections or merely the predilection of the organism for more severely damaged airways is uncertain. Of the several risk factors for developing a P. aeruginosa pulmonary infection (including chronic obstructive pulmonary disease [COPD], malnutrition, mechanical ventilation, steroid therapy), prolonged hospitalization is one of the most important. The radiographic pattern resembles bronchopneumonia with lobular, segmental, or lobar involvement and no consistent zonal distribution. 37 The reported frequency of abscess formation or cavitation is variable but is probably low (<20%) compared with Gram-positive bacterial infections. Similarly empyema seems to be a relatively uncommon complication. On CT a tree-in-bud pattern or centrilobular nodulation is present in half of patients with nosocomial P. aeruginosa infection. 81 Bilateral pleural effusions were common (46%) in this series. 81
Klebsiella pneumonia
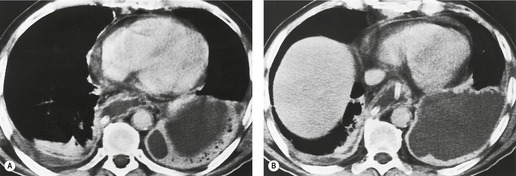
Pneumonia caused by K. pneumoniae, like the other Gram-negative pneumonias, usually affects people with chronic debilitating illnesses or alcoholism. The symptoms include high fever and toxemia and clinically resemble those of severe pneumococcal pneumonia. On chest radiography the consolidations are also similar to those seen with S. pneumoniae pneumonia: the disease is often confined to one lobe, with homogeneous nonsegmental consolidation that spreads rapidly to become a lobar pneumonia. Multilobar and bilateral consolidations may occur. Much was made of lobar expansion in early series,82. and 83. but this feature is unusual in the modern antibiotic era. However, expansion of consolidated lobes on CT was reported in 6/11 patients. 84 In addition, the consolidation was described as consisting of two intermingled parts: enhancing areas and poorly marginated low-attenuation areas, the latter containing small air cavities suggesting necrosis.
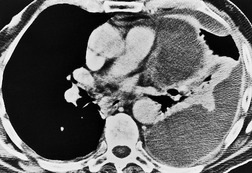
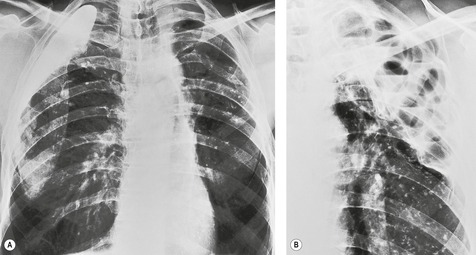
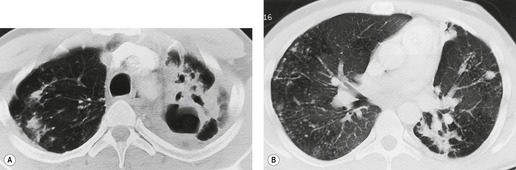
Cavitation, which may occur early and progress quickly, is seen in 30–50% of cases on chest radiography (Fig. 5.26). This feature distinguishes Klebsiella pneumonia from pneumococcal pneumonia, in which cavitation is rare. The cavities are frequently multiple (Fig. 5.26) and may attain great size. Solitary large chronic abscesses are occasionally encountered. 85 Massive necrosis, so-called pulmonary gangrene, is a rare but recognized phenomenon. Pleural effusion and empyema are reportedly uncommon in an early series, 68 but in another study effusions were identified in 8/11 patients. 84
Legionnaires disease is regarded as one of the atypical pneumonias. 86 It results in severe pneumonia with a high mortality, although this has markedly decreased in recent years. 87L. pneumophila is an aerobic Gram-negative bacillus found in aquatic environments such as reservoirs, cooling towers, water distribution systems, and humidifiers. 88 Other Legionella species lurk in artificial aqueous environments and can also cause pneumonia. 89 Infection comes from these sources rather than from person-to-person contact. The disease may be sporadic or occur in localized epidemics centered on an infected water source;90. and 91. the most notable example was the 1976 outbreak at an American Legion convention, in which 29 of 182 affected delegates died, 92 hence the name ‘legionnaires disease’. The infection is characterized by malaise, myalgia, headache, abdominal and chest pain, nausea, vomiting, diarrhea, high fever, rigors, dyspnea, and cough; the cough is usually productive and associated with hemoptysis. Bacteremic dissemination causes a variety of extrapulmonary manifestations, including endocarditis, sinusitis, brain abscess, and pancreatitis. Predisposing chronic diseases are common and may be either pulmonary, such as chronic bronchitis and emphysema, or systemic, such as malignant disease or renal failure. Coinfection with another bacterium, such as S. pneumoniae, is not uncommon. 93 Corticosteroid therapy is a recognized risk factor, but surprisingly patients with neutropenia or acquired immune deficiency syndrome (AIDS) do not appear to have an undue predilection for legionnaires disease. 88 The organism is difficult to culture from sputum and blood, but a Legionella urinary antigen test is increasingly being used. 94 Nevertheless the diagnosis remains presumptive in many cases. 86
The radiographic appearances have been reviewed in detail by Fairbank and associates. 95 The initial finding is peripherally situated patchy consolidation (Fig. 5.27), which spreads rapidly, often involving more than one lobe and becoming bilateral in half the cases (Fig. 5.28). There may be a predilection for the lower lobes, 96 but this is not seen in all series. 97 The consolidation may assume a spherical configuration or may coalesce to resemble lobar pneumonia.27. and 98. Cavitation, although reported, is unusual (Fig. 5.28); 99 it appears to be most common in immunocompromised patients.97. and 100. Pleural effusions, which are usually small but occasionally massive, are documented with variable frequency (10–66%)91.97. and 99. and frank empyema formation may rarely occur. 101 Unusual radiographic features include hilar adenopathy and spontaneous pneumothorax. 95 An unusual pattern of multiple 0.5–2 cm pulmonary nodules has been reported in an infant. 102 Radiographic resolution is slow, particularly in immunocompromised patients, and lags behind the clinical improvement. The radiographic changes usually persist for at least a month after the acute illness. CT adds little to the diagnosis of Legionella pneumonia, but interestingly may show pulmonary abnormalities in about half of infected individuals without respiratory symptoms; 103 multiple segment consolidation may show adjacent ground-glass opacification. A peculiar feature is the apparently persistent nature of some of the pulmonary abnormalities104. and 105. with symptoms still present up to 19 months after presentation; apart from the finding of bronchiectasis the high-resolution CT (HRCT) features are not clearly documented and the nature of these convalescent or persisting abnormalities is uncertain.
L. micdadei pneumonia is considered separately in the section on immunocompromised patients on p. 322.
Pertussis (whooping cough)
Whooping cough is caused by the aerobic Gram-negative coccobacillus Bordetella (Haemophilus) pertussis. Pneumonia caused by this organism is uncommon in communities with a high uptake of immunization. 106 Pneumonia occurs approximately four times more frequently in adults over the age of 30 years than in younger individuals107 and pertussis may be the cause of a troublesome cough in elderly people. 108 In previously immunized individuals the clinical course is usually milder, with persistent cough being a prominent and distressing symptom. 109
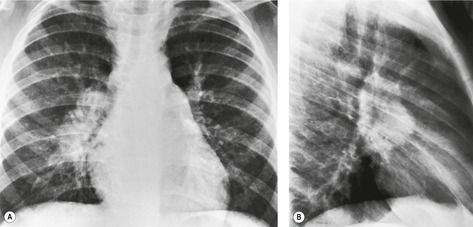
On chest radiographs110.111. and 112. the striking feature is extensive peribronchial consolidation in one or more lobes. A large series, comprising 238 patients ill enough to require admission to the hospital, provides a good indication of the chest radiographic findings. 111 Sixty-three patients (26%) had abnormal findings on chest radiography. Pulmonary consolidation, which was predominantly peribronchial in distribution, was present in 50 patients, pulmonary collapse in nine, and visible lymphadenopathy in 22. The pulmonary changes showed a tendency to involve the right lung, particularly the lower and middle lobes. The peribronchial consolidation tends to be maximal close to the mediastinum, giving rise to an appearance that has been dubbed the ‘shaggy heart sign’ (Fig. 5.29). 110 This distribution seems to be mirrored by the location of postpertussis bronchiectasis (which is said to have a predilection for the right middle lobe and lingula).
Brucellosis, an infection transmitted by inhaling infected material from domestic animals, particularly cows, pigs, and goats, or by ingesting infected animal products, such as raw milk, only occasionally causes pneumonia. The responsible organism is a Gram-negative coccobacillus. The symptoms include those of systemic infection: fever, joint pains, malaise, and headache. 113 Multisystem involvement with protean symptoms is common, so that diagnosis may be elusive. 114 Symptoms of pneumonia occur in a minority of cases (4% in one series, 113 10% in another). 115 Pneumonia as the sole manifestation of brucellosis is extremely uncommon. 116 The findings are of areas of consolidation, hilar and paratracheal adenopathy, nodular or miliary shadowing, and pleural effusions.115. and 117. Spherical calcifications surrounded by thin lamellar calcifications may be seen in the spleen as a late manifestation.117. and 118.
Melioidosis
Melioidosis119 is due to the aerobic Gram-negative bacillus Burkholderia pseudomallei, an organism that resides in dust and soil. Pneumonia is rare except in the flooded fields (e.g. post-tsunami) and marshes of southeast Asia, 120 but cases occur in Australia and nontropical countries.121. and 122. Multiple organ involvement is common, with the lungs the most frequently affected organ.120. and 123. The acute form, which can be rapidly fatal (~80% mortality rate), is characterized by positive blood cultures, fulminating septicemia, and high fever, with or without acute respiratory failure. 124 The subacute form consists of cough, which is usually productive, occasional hemoptysis, low-grade fever, weight loss, and pleuritic chest pain. In some patients few symptoms occur and melioidosis is diagnosed only because pulmonary disease is found on chest radiography. Patients with cystic fibrosis may be more than usually susceptible to chronic melioidosis. 125
On chest radiographs120.123.126.127. and 128. the acute pneumonia shows small, round, ill-defined areas of consolidation that are often unilateral and may coalesce to form segmental or lobar opacities (Fig. 5.30), with an affinity for the upper lobes. 129 Cavitation may occur. Pleural effusion, empyema, 130 and pneumothorax are seen in a small proportion of patients, 120 and hilar adenopathy has been reported.
In the subacute form the chest radiograph shows a variety of patterns, including round, segmental, or lobar consolidation, which often cavitates.120. and 128. In the chronic subclinical forms the chest radiograph closely resembles postprimary tuberculosis with patchy upper lobe consolidation and cavitation. 129 Melioidosis is relatively resistant to antimicrobial therapy and the relapse rate is high. 122
Plague
Plague is due to Yersinia (Pasteurella) pestis, a Gram-negative coccobacillus still found in some areas of Asia, Africa, South America, and southwestern USA.131.132. and 133. Pneumonia may be primary, resulting from inhalation of infected droplets, or may spread hematogenously from infected swollen axillary or femoral lymph nodes, sometimes known as buboes. The resulting pneumonia is fulminant, with high fever, and death is inevitable without appropriate antibiotic treatment. 134 In fatal cases numerous petechiae and ecchymoses develop, the appearance of which give rise to the name ‘Black Death’ in the fearful epidemic that swept Europe in the fourteenth century. Because of its virulence it is regarded as a potential agent for bioterrorism. 135
Chest radiography131. and 136. shows rapidly progressive dense patchy consolidations that may be nodular, segmental, or lobar in shape. Eventually multiple lobes are involved and mediastinal adenopathy and pleural effusions may develop. In some cases, mediastinal and hilar adenopathy is the only radiographic finding.
Pasteurella multocida is a Gram-negative rod or coccobacillus that infects cats and dogs. Respiratory infection resulting in acute bronchitis, bronchopneumonia, lung abscess, or empyema may follow inhalation of organisms or a bite. The radiographic changes include lobar, multilobar, or widespread patchy consolidation, usually sparing the upper lobes. 136 Pleural effusions occur in up to 20% of patients.
Tularemia
Tularemia, named after Tulare County in California, is due to Francisella tularensis, an aerobic Gram-negative coccobacillus. The disease is endemic in many parts of the world, including Europe, Asia, and North America. Human infection is acquired in a variety of ways:
• Through the skin in individuals who handle infected animals (rabbits, squirrels, skunks, dogs, game birds, and many others) or their skins
• By bites from infected insect vectors, notably ticks, or mosquitoes, fleas (the latter were thought to be responsible for an outbreak in Sweden137)
• By bites from the infected animals themselves
• By inhalation of organisms from infected carcasses or even the inhalation of particles produced by lawn mowing (!), 138 of dust, or following laboratory accidents. Pneumonia is a common finding in patients with tularemia.
The radiographic signs of tularemia pneumonia are lobar, segmental, rounded, oval, or patchy pulmonary consolidations, which may be unilateral or bilateral in distribution (Fig. 5.31).139. and 140. The most common pattern is unilateral patchy consolidation, but widespread bronchopneumonia, lobar consolidation, a pattern resembling pulmonary edema, lung abscess, and apical opacities resembling tuberculosis are all encountered. 136 Cavitation may occur but is unusual. Miliary nodulation was reported in one case in a large series. 140 The pulmonary changes may be accompanied by cardiomegaly caused by pericarditis with pericardial effusion. Hilar and mediastinal adenopathy is common141 as are pleural effusions, both of which may be unilateral or bilateral. Empyema and bronchopleural fistula may supervene. On rare occasions the consolidation resolves with fibrosis and calcification, resembling tuberculosis and histoplasmosis.
Most anaerobic lung infections result from aspiration of infected oral contents, and obvious periodontal disease is present in many patients.20.142.143. and 144. Predisposing factors such as a recent episode of altered consciousness, dysphagia, or alcoholism are frequent.20. and 142. Anaerobic infections are second only to S. pneumoniae as a cause of community-acquired pneumonia requiring hospitalization.
The radiographic appearances142. and 145. can be conveniently divided into pulmonary consolidation with (up to 40%) or without cavitation, and discrete lung abscess, each of which may be associated with empyema. Anaerobic pneumonia has a predilection for the lower lobes (Figs 5.1 and 5.32), with the right lung more commonly affected than the left. These sites are compatible with the idea that the pneumonia follows aspiration from the upper respiratory tract. There is usually one predominant focus of disease, but multilobe involvement is also common (Fig. 5.33).
Discrete lung abscesses occur chiefly in the posterior portions of the lungs, usually in the posterior segments of the upper lobes (Fig. 5.34) or in the superior segments of the lower lobes. In patients with cavitation the disease takes longer to resolve, sometimes 2 months or more. Hilar and mediastinal adenopathy may accompany lung abscess, 147 and such cases may therefore resemble carcinoma of the lung.
A third to half of patients have empyema.142. and 145. Over half the patients in one series of anaerobic bacterial empyema had no apparent parenchymal disease. 145 If pleural effusion is seen in association with anaerobic lung infection, it is virtually certain to be an infected empyema. 145 The infected fluid is frequently loculated. Very large empyemas may develop and bronchopleural fistula is a recognized complication.
Syphilis
Pulmonary infection caused by Treponema pallidum is rare, and reports are scanty.148. and 149. Diffuse bronchopneumonia, diffuse pulmonary fibrosis, and solitary or multiple pulmonary nodules have been reported.150. and 151.
Pneumonic consolidation occurs in a fifth to two-thirds of patients with leptospirosis.152.153. and 154. It seems that a history of cigarette smoking may increase the risk of developing pulmonary leptospirosis. 155 The pulmonary consolidation represents hemorrhagic pneumonitis, 156 which may be fatal in a high proportion of cases. 157 Although one series has reported acute lung injury in 42 ventilated patients with leptospirosis, it seems probable that, in the absence of other reports, the pulmonary involvement in these cases was the expected extensive hemorrhage. Chest radiographs152.158.159. and 160. show bilateral, multiple areas of pulmonary consolidation that may take the form of multiple well-defined small nodules or multifocal nonlobar consolidations with a tendency towards a peripheral predominance. These patchy areas of consolidation in severe cases may be extensive and confluent. Patchy discoid atelectasis and small pleural effusions are common. Interlobular septal thickening has been noted in a small proportion of patients. 152 Hilar and mediastinal adenopathy does not appear to be a feature.
The HRCT findings are, as might be anticipated from the pathology of extensive pulmonary hemorrhage, widespread ground-glass opacification and consolidation, 161 with some poorly defined centrilobular and acinar nodules. There are no ancillary features to suggest leptospirosis as the cause of these nonspecific abnormalities.
Rickettsial infections
The most common rickettsial pneumonia is Q fever, caused by C. burnetti.162 Q fever occurs worldwide and is acquired from infected dust, from cattle or sheep products, or occasionally from the bite of infected ticks or mites. The disease occurs sporadically and in epidemics.163. and 164. The symptoms are sudden in onset and include a flulike illness with fever, dry cough, myalgias, arthralgias, and headache. Pneumonia develops in less than half those infected. Many different organs, particularly the heart, 165 may be involved, and it seems that younger patients are more prone to hepatitis whereas older, possibly less immune competent, individuals, 166 or those with chronic airways disease,167. and 168. are more likely to develop pneumonia. Prognosis is good apart from those with myocarditis or meningoencephalitis.
The usual radiographic appearance of Q fever pneumonia (Fig. 5.35)29.169.170. and 171. is unifocal or multifocal, subsegmental, segmental, or lobar consolidation. Typically, there is a single segmental opacity in an upper lobe, 171 but in general the radiographic findings are entirely nonspecific. 172 Spherical (round) pneumonia is also reported particularly in epidemic cases.173. and 174. Very occasionally these round pneumonias are confused with lung cancer. 173 Cavitation is rare. 175 Pleural effusions are seen in some patients, particularly in sporadic infection. CT abnormalities largely reflect radiographic findings, namely multifocal consolidation (Fig. 5.36). However, in a series of 12 patients, one patient had nodular lesions, some of which had a ground-glass halo which, the authors suggested, might represent angio-invasion176 (although evolving septic embolism is an alternative explanation) (Fig. 5.36). Lymphadenopathy and small pleural effusions are more readily disclosed on CT. The disease is self-limiting, but resolution of pulmonary consolidation may take up to 6 months; 172 the average time is 39 days. 171
(With permission from Voloudaki AE, Kofteridis DP, Tritou IN, et al. Q fever pneumonia: CT findings. Radiology 2000;215:880–883. Copyright Radiological Society of North America.)
Rocky Mountain spotted fever, caused by Rickettsia rickettsii, is encountered mostly in southeastern USA, where it is transmitted through tick bites. It is an acute, often fulminant, disease in which small vessel inflammation is the basic pathologic process. The vasculitis is clinically most evident in the skin and central nervous system. In the lungs the resulting pulmonary vasculitis leads to a variety of patterns, varying from unifocal or multifocal consolidations, resembling bacterial pneumonia, to widespread pulmonary infection, resembling pulmonary edema, combined in some cases with pleural effusions.177. and 178. The pathologic result is interstitial and alveolar edema and hemorrhage, together with a mononuclear and lymphocytic interstitial infiltrate. 179 Bacterial superinfection appears to be rare. 178 The clinical diagnosis depends on recognizing a multiorgan vasculitis, notably of the skin and meninges, in an acutely febrile patient during the tick season in endemic areas. The mortality is high in patients with widespread pulmonary consolidation. Myocardial involvement is a rare manifestation. 180
Chlamydial infections
C. psittaci infection, so-called ornithosis or psittacosis, is usually acquired from infected birds. 181 Infection with the psittacosis agent may result in disease of wide clinical spectrum, ranging from completely asymptomatic infections recognized only by serologic means to respiratory failure182 or overwhelming illness involving multiple organ systems. 183 Usually the patient complains of fever, malaise, headache, and a nonproductive cough, and the clinical picture may be indistinguishable from other acute bacterial pneumonias. The chest radiograph reveals patchy pulmonary consolidation (Fig. 5.37), which can be extensive. Another described pattern is patchy reticular shadowing with lower zone predominance that appears more severe than would be expected from the clinical features. Pleural effusions have been reported in up to 50% of cases, but are usually small. 184
Chlamydia trachomatis is a cause of pneumonia in neonates and infants, in whom it may cause widespread streaky consolidations and air trapping similar to that seen with acute bronchiolitis of viral origin. 185 In a few reported cases in adults the chest radiographs showed focal streaky consolidation without evidence of air trapping. Pleural effusion, although reported, is not a striking feature.186. and 187.
Chlamydia pneumoniae is an underrecognized cause of community-acquired pneumonia, accounting for perhaps as many as 10% of cases of pneumonia in adults.188. and 189. Antibody responses to C. pneumoniae are highly variable, making serologic studies of its prevalence difficult. Infection with C. pneumoniae may be confined to the upper respiratory tract but pneumonia of variable severity occurs in approximately half of cases. The radiographic manifestations range from focal airspace consolidation to widespread interstitial shadowing; indeed, C. pneumoniae has been suggested as a pathogenetic agent of nonspecific interstitial pneumonia (NSIP). 190 There seem to be differences in the radiographic appearances between first exposure infections and previously exposed individuals: 191 recurrent infections tend to be characterized by more widespread interstitial shadowing. As with other pulmonary chlamydial infections, pleural effusions occur in some patients. 192 Two CT studies have documented appearances that are similar to pneumonias caused by M. pneumoniae or S. pneumoniae,48. and 193. although bronchial wall thickening and airway dilatation seem to be more frequent in C. pneumoniae pneumonia.
The most common sources of septic pulmonary emboli are infected venous catheters, including pacemaker wires; tricuspid valve endocarditis (a major source in intravenous drug users); 194 septic thrombophlebitis (again a significant problem in drug addicts); and indwelling prosthetic devices. Immunocompromised patients are particularly vulnerable. Although rare, anaerobic infection of the lateral pharyngeal space sometimes leads to suppurative jugular vein thrombosis and septic pulmonary emboli (Lemierre syndrome).195. and 196.
• Many potential sources, but may occur in the absence of septicemia or obvious infected source
• Distribution and morphology best appreciated on CT
• Often nonspecific in shape but often cavitate and abut a pleural surface
• A ‘feeding vessel’ present in only a minority of septic emboli
• Accompanying pleural effusion/empyema common
The diagnosis is usually established by positive blood cultures and the presence of an infected source for the emboli. It is worth noting that positive radiographic findings, particularly abnormalities seen on CT, may be present before blood cultures become positive, 197 and the diagnosis may be first suggested at chest CT. 198
The usual radiographic and CT appearances197. and 198. consist of multiple pulmonary opacities. As usual, CT shows more lesions and enables the radiologist to characterize these lesions with greater accuracy than is possible from plain chest radiographs. The opacities may occur in any portion of the lungs but are usually maximal in the lower zones. The lesions are usually either round (nodular) in shape or show the expected shape of a pulmonary infarct, namely a wedge-shaped density based on the pleura and pointing to the hilum. Sometimes, however, the opacities are completely nonspecific in shape. They may be any size and frequently cavitate (Fig. 5.38), a feature more easily recognized at CT. For example, in the series by Kuhlman et al., 197 50% of the visible nodules showed cavitation. Air bronchograms are frequently seen, particularly at CT, in all types of opacity, including the nodular lesions. It has been suggested that there may be differences in the characteristics of septic emboli caused by Gram-negative and -positive bacteria; 199 Gram-positive emboli tended to be larger and cavitate more readily, but confirmation of such differences in a larger series is needed. The ‘feeding vessel sign’, a vessel leading to the apex of a peripheral area of consolidation, has been reported as a useful sign in the context of septic emboli.197.198. and 200. However, Dodd et al. 201 have convincingly demolished, with the use of multidetector CT reformats, the impression that vessels ‘feeding’ septic emboli are a useful sign: on reformatted images less than 15% of lesions show a vessel apparently entering the spherical- or wedge-shaped opacity, and several such vessels could be traced to the left atrium (i.e. they represent pulmonary veins). The combination of multiple peripheral nodules or wedge-shaped consolidations, some of which have cavitated, in the appropriate clinical setting is highly suggestive of the diagnosis of septic emboli.197. and 198. Accompanying pleural effusion and empyema is a common feature.197. and 198.
Intraluminal filling defects in the pulmonary arteries are not an expected feature, because septic infarcts are almost invariably the consequence of very small infected emboli that lodge in the distal pulmonary vasculature.
BACTERIAL PARAPNEUMONIC PLEURAL EFFUSIONS AND EMPYEMA
The distinction between a sterile parapneumonic pleural effusion and an infected collection (empyema) is often impossible. For conclusive proof of an empyema, positive pleural fluid cultures are needed. Up to 40% of hospitalized patients with pneumonia develop an effusion202 and, whether infected or not, consideration needs to be given to whether the pleural effusion is likely to resorb or have a protracted course. 203 The terms complicated versus uncomplicated parapneumonic effusion are largely based on the distinction that a complicated effusion will usually require interventional treatment of some kind. 204 The spectrum and timing of treatment options are wide, and range from the conservative through tube drainage with instillation of a fibrinolytic agent205 to aggressive surgical intervention for a severe multiloculated empyema.206. and 207. The ability of imaging features alone to predict the need for surgical versus medical management is limited.208. and 209.
Most empyemas are associated with a recognizable pneumonia, surgery, trauma, or infradiaphragmatic infection.211.212. and 213. The bacteria usually responsible for nontuberculous empyemas or ‘parapneumonic’ effusions are anaerobic bacteria, S. aureus, S. pneumoniae, other streptococcal species, and various Gram-negative bacteria. 214 A positive microbiological yield from aspiration of a parapneumonic effusion is obtained in between 20% and 70% of cases,215.216.217. and 218. and the extent to which routine microbiologic analysis of a pleural effusion changes management has been questioned. 215
The clinical picture of patients with bacterial pneumonia and pleural effusion is similar to that of patients with pneumonia alone. Patients with anaerobic bacterial infections of the pleural space usually present with a subacute illness. The majority have a history of alcohol misuse, an episode of unconsciousness, or another reason for aspiration.
The diagnosis of parapneumonic effusion and empyema depends on recognizing the presence of fluid in the pleural cavity and aspiration of a sample for analysis. Because empyemas are rich in protein, the pleural fluid tends to loculate and therefore ultrasound or CT may be necessary to appreciate the full size of the pleural fluid collection. As a generalization, smaller volumes of fluid clear with antibiotic treatment, and therefore thoracentesis is not required.202. and 210.
The appearance on plain chest radiographs (Fig. 5.40, Fig. 5.41 and Fig. 5.42) 212 varies with the evolution of the parapneumonic fluid collection. Uncomplicated, sterile effusions appear identical to pleural fluid collections that may accompany noninfectious consolidations. Previous scarring of the pleural cavity may lead to loculation, but otherwise the fluid is mobile. Fibropurulent fluid collections have a predictable tendency to loculate.
The distinction between pulmonary consolidation or abscess and infected loculated pleural fluid on conventional films can occasionally be difficult but has important therapeutic consequences. The radiographic features to be analyzed are shape and the appearance of any air within the opacity. 219 The shape is often the most definitive feature. Loculated collections of pleural fluid, with the exception of interlobar fluid, are based on the parietal pleura and cause an oval, lens-shaped, or rounded expansion of the pleura (Fig. 5.40). When profiled the inner margin of the empyema is sharply defined and shows a curved, smooth interface with the adjacent lung, but often one or more interfaces with the lung are not tangential to the beam and the empyema therefore has an imperceptible border. Round pneumonias do not show the very smooth, well-defined interface with the adjacent lung that is seen with empyemas. Also, although they may contact the pleura, round pneumonias are rarely as broadly based on the pleura.
Interlobar loculated pleural fluid has a unique radiographic appearance. The opacity is centered on a fissure and is lens shaped with a more pronounced bulge inferiorly than superiorly, reflecting the gravitational effect of the fluid suspended within the fissure. In the lateral projection, interlobar fluid in the major fissure appears as a well-defined lens shape, whereas in frontal projection the opacity is circular and fades off in all directions. It is therefore in the frontal view that confusion with pneumonia is most likely to occur.
If an air–fluid level is present, the comparative length in frontal and lateral projections may help distinguish lung abscess and empyema (Fig. 5.41). Since empyema spaces are usually lenticular in shape, the air–fluid level is often substantially longer in one view than in the other (compared with the spherical cavity of an abscess which has the same length of air–fluid level regardless of projection). Also, in empyema the air–fluid level may reach the chest wall, whereas a lung abscess is often surrounded by lung parenchyma, and the air–fluid level is therefore less likely to touch the chest wall.
• Shape. Empyemas, unless very large, are basically lenticular in shape. The angle formed at the interface with the chest wall is obtuse or tapering. Large collections, however, may be more spherical and may then show acute angles. Lung abscesses, on the other hand, tend to be spherical and show acute angles at their margins with the chest wall. Also, fluid collections in the pleural space may change their shape as the patient changes position, whereas lung abscesses are fairly rigid and retain approximately the same shape in upright, supine, prone, or decubitus views.
• Wall characteristics. The wall of an empyema is formed by thickened visceral and parietal pleura. This thickened pleura is uniform in thickness and soft tissue density, with a smooth inner and outer edge enclosing the empyema fluid; this combination of findings has been called the split pleura sign. 220 The increased thickness of the parietal pleura is particularly easy to appreciate and is not a feature of a transudate collection. 226 Normally the combined thickness of visceral and parietal pleura, together with the adjacent innermost intercostal muscle, is less than 1–2 mm. In empyemas the parietal pleura alone is 2–5 mm in some 80% of cases. 227 The thickened pleura enhances following the administration of intravenous contrast medium in almost all cases.209. and 227. The wall of a lung abscess usually has an irregular inner and outer margin. It also tends to be thicker than the wall of an empyema, may contain multiple dots of air, and may on occasion even show distorted air bronchograms.
• Fluid contents. The density characteristics of the empyema fluid are generally uninformative. Small bubbles of gas are a frequent finding (58% in one series), 228 but their significance is usually uncertain; they are more likely to reflect the consequence of air introduced by thoracentesis than the production of gas by anaerobic bacteria.
The extrapleural fat adjacent to an empyema is often increased in width, and the widened fat line may show increased attenuation believed to be due to inflammatory changes in the fat, 227 especially in chronic tuberculous empyemas. 229 Similarly, the muscles of the chest wall may be swollen because of edema. 212 Moderately enlarged mediastinal lymph nodes are identifiable in approximately a third of patients with an empyema or parapneumonic effusion, 230 but these are rarely greater than 2 cm in diameter.
Malignant neoplasms may arise in the walls of chronic, longstanding empyema cavities; this association appears to be highest in tuberculous empyemas but is also encountered in nontuberculous infection. 231 The range of neoplasms is wide and includes non-Hodgkin lymphoma, squamous cell carcinoma, mesothelioma, and rarely sarcoma. 231 The diagnosis of neoplasm in a chronic empyema can be difficult even with CT,221. and 231. because neoplastic tissue and chronic pleural inflammatory disease both have the same density and because nodularity is seen with chronic infection as well as neoplasm. MRI may show a difference in signal intensity between mature fibrous tissues and neoplastic tissue, 231 but the diagnostic accuracy of this difference is unknown.
Tuberculosis remains a worldwide scourge232 and was a leading cause of death in the USA at the turn of the twentieth century; the global prevalence of M. tuberculosis has been estimated to be 32%. 233 Improved public health measures and specific antituberculous chemotherapy dramatically reduced the prevalence of tuberculosis, and near eradication of the disease once seemed likely. In 1985, some 22000 new cases were reported in the USA, representing the lowest incidence since national reporting began in 1953. 234 However, in the 1990s the incidence of tuberculosis began to increase again. The increase was widely attributed to the HIV epidemic. HIV-infected individuals, particularly intravenous drug users, are at considerable risk for reactivation of tuberculosis. 235 Nevertheless, the highest case rate for tuberculosis occurs in people over 65 years of age, a group by and large not involved in the HIV epidemic. Tuberculosis in the elderly usually represents reactivation of previously acquired disease as a result of waning immunocompetence with advancing age. 236 These individuals acquired the disease at a time when it was more prevalent than it is today. Tuberculosis remains a considerable health problem in developing countries and the USA and Europe have seen a considerable influx of immigrants and refugees from these countries in recent decades. Approximately a quarter of new cases of tuberculosis in the USA involve patients born outside the country, 236 and, in the UK, currently two-thirds of new cases occur in immigrants. 237 Tuberculosis is now more obviously an urban disease, involving deprived population groups especially; the incidence is high in prison populations and among the indigent and the homeless. 238 Classic pulmonary tuberculosis is readily diagnosed, but increasingly tuberculosis is encountered in the elderly, who may have other serious medical problems, making the diagnosis more challenging. Furthermore, tuberculosis in adults is increasingly a primary infection and by no means classic ‘adult’ tuberculosis. A key factor in diagnosis of tuberculosis is simply awareness that this disease still lurks. Almost all cases are caused by infection with the human strain of M. tuberculosis and the remainder by the atypical mycobacteria, notably Mycobacterium kansasii and Mycobacterium avium–intracellulare.
• Endobronchial tuberculosis – ulcers and strictures, bronchial obstruction leading to collapse or hyperinflation, bronchiectasis
• Involvement of the pleura – diffuse pleural thickening, effusions, pneumothorax, bronchopleural fistula, eventually calcified pleural thickening
The inflammatory response to tuberculous infection differs from the usual inflammatory response to infecting microorganisms in that it is modified substantially by a hypersensitivity reaction to components of the tubercle bacillus. The extent to which the hypersensitivity reaction is advantageous to the host, or deleterious in resisting the infection, is uncertain. Cellular immunity involving activated macrophages has an important role in containing and combating tuberculosis. When cellular immunity is impaired by disease or treatment-related immunodeficiency or when pulmonary macrophages are damaged, for example by silica exposure, resistance to M. tuberculosis is reduced.
Various terms are applied to the form of tuberculosis that develops and progresses under the influence of established hypersensitivity. These terms include postprimary, secondary, or reactivation tuberculosis. The term ‘reactivation tuberculosis’, although not ideal because the disease sometimes evolves from primary tuberculosis without a latent interval, does serve to emphasize that most cases represent reactivation of endogenous infection rather than reinfection with M. tuberculosis. 238 Postprimary or reactivation tuberculosis develops under the immediate influence of hypersensitivity, which accelerates the changes described previously. In particular, caseous necrosis occurs at an early stage in the process. Involvement of the regional lymph nodes is not a typical feature of reactivation tuberculosis; whether this is by virtue of the hypersensitivity reaction or acquired immunity is uncertain. Factors that predispose to reactivation of tuberculosis include aging, malnutrition, uremia, diabetes mellitus, alcoholism, silicosis, cancer, familial and acquired immune deficiency diseases, and drug-induced immunosuppression. 235
The gross morphologic features of reactivation tuberculosis239 can be subdivided into the following:
1. The foci of acute tuberculous infiltration in the pulmonary parenchyma.
2. Cavity formation. Airspaces in a tuberculous process may represent excavated foci of caseous necrosis or, alternatively, pneumatoceles or bullae that follow fibrous contraction or endobronchial disease.
3. Fibrosis and distortion of lung architecture. The extent of the fibrosis and damage to the lung depend on such factors as the amount of caseous necrosis and the severity of associated endobronchial and pleural disease. Fibrous tissue contracts as it matures, and even quiescent lesions may show increased contraction and distortion over an extended period of observation.
4. Calcification. Dystrophic calcification often occurs in foci of caseous necrosis. Such calcification takes considerable time to become radiographically visible and is often associated with pulmonary fibrosis (fibrocalcific disease) or tuberculoma formation.
5. Tuberculoma formation. Namely a focus of tuberculosis in which the processes of activity and containment are finely balanced. The result is a fairly discrete nodule or mass in which repeated extensions of infection have created a core of caseous necrosis surrounded by a mantle of epithelioid cells and collagen with peripheral round cell infiltration.
Both primary and reactivation tuberculosis may extend to extrathoracic sites such as the gastrointestinal tract, larynx, kidneys, bones, joints, and central nervous system. In these cases it is generally thought that the primary portal of entry is the lungs, even though in many instances there is no radiographic evidence of pulmonary tuberculosis. Tuberculosis of the larynx and tuberculosis of the gastrointestinal tract have a high association with visible active pulmonary tuberculosis. 240
Radiographic appearances of pulmonary and pleural tuberculosis
Tuberculosis may involve the lungs in disease patterns that reflect a number of factors: the host’s immune status, the existence of hypersensitivity from previous infection, the method of spread of disease, and an incompletely understood tendency of the disease to affect certain portions of the lungs. The relationship between the radiographic pattern of disease and the time at which tuberculosis was acquired is probably less clear than previously thought. 241 However, the radiographic appearances can be considered under the following broad headings:
• Primary tuberculosis
• Reactivation (postprimary) tuberculosis
• Focal pulmonary tuberculosis
• Tuberculous lobar pneumonia and bronchopneumonia
• Endobronchial tuberculosis
• Tuberculoma formation
• Miliary tuberculosis
• Tuberculous pleuritis.
These very broad patterns of disease may overlap or undergo transformation from one to another.
Primary tuberculosis
Formerly the initial infection with M. tuberculosis usually occurred in childhood, but primary tuberculosis has been increasingly encountered in an adult population. In one series242 over half the cases of primary tuberculosis occurred in individuals 18 years of age or older and a quarter of adult cases were deemed to represent the primary form of the disease. The division between primary tuberculosis and postprimary or reactivation tuberculosis is by no means clear-cut; a minority of cases of primary tuberculosis may evolve without any interval into a chronic progressive form of the disease indistinguishable from reactivation tuberculosis (this is sometimes called progressive primary tuberculosis). Classically the tubercle bacillus causes a nonspecific focal pneumonitis (Fig. 5.47). In approximately half of cases the primary pulmonary foci are never identified or documented. 243 Indeed the chest radiograph may remain entirely normal despite definite conversion of tuberculin sensitivity or the presence of positive sputum cultures. 244 The predominant radiographic feature of primary tuberculosis is the presence of adenopathy in the appropriate lymph drainage pathways (Figs 5.47 and 5.48). In one series radiographic evidence of lymphadenopathy was found in 92% of 191 children with primary tuberculosis. 243 A focus of tuberculous pneumonia (termed a Ghon focus) when detected radiographically is almost invariably associated with lymphadenopathy. The resultant hilar adenopathy is usually unilateral, and any mediastinal adenopathy is contiguous to the affected hilum. In some patients hilar adenopathy is bilateral or mediastinal adenopathy occurs alone. 245 The adenopathy may be strikingly severe and extensive, particularly in individuals of African or Asian origin (Fig. 5.49), and may closely resemble lymphoma, metastatic disease, or sarcoidosis. In middle-aged and elderly patients lymph node enlargement is less common and usually less apparent than it is in children.
The pulmonary foci of primary tuberculosis are randomly distributed and range from small ill-defined parenchymal shadows to segmental or lobar consolidation. Curiously, there appears to be a predilection for involvement of the right lung. 243 Slight expansion of consolidated lobes may be noted. In the absence of cavitation, consolidation of segments or lobes produces a radiographic picture indistinguishable from that of the bacterial pneumonias. The time course is, however, different; tuberculous pneumonia is much more indolent, often taking weeks or months to clear. Primary tuberculosis may be masslike and in an adult may be confused with such conditions as Wegener granulomatosis or a pulmonary neoplasm (Fig. 5.50). A single pulmonary focus occurs in most instances, but multiple foci may be encountered. The reported incidence of cavitation varies, but is unusual and probably occurs in less than 15% of cases (Fig. 5.51). The pulmonary focus frequently resolves without trace, or alternatively it may evolve into a small nodule or scar that may then calcify. Such calcifications may be observed following primary tuberculosis in up to 20% of patients (Fig. 5.52). Hilar or mediastinal lymph node calcification is observed in up to a third of cases. Single or multiple tuberculomas may develop in primary tuberculosis, but they are seen much less frequently than in reactivation tuberculosis.
Pleural effusions occur in primary tuberculosis. In these cases, which have been studied in a hospital setting, pleural effusions have been observed in approximately a quarter. On the other hand, Leung and associates, 243 studying an unselected series ranging from completely asymptomatic patients to one with a tuberculous empyema, found pleural effusions in only 6%. The effusions are generally unilateral and are usually associated with some identifiable pulmonary parenchymal abnormality. Segmental or lobar airway narrowing is frequent and may be caused by endobronchial tuberculosis or by extrinsic pressure from enlarged lymph nodes. 246 The result is usually segmental or lobar atelectasis, but air trapping occurs occasionally (Fig. 5.53). 247
CT is capable of considerable precision in the investigation of primary tuberculosis, although in most cases it is unnecessary. CT may identify foci of disease in the lung undetected on plain radiography and thereby assist the bronchoscopist in questionable cases. 248 Occult cavitation may be detected, particularly when obscured by a pleural effusion. Bronchial stenoses, bronchial occlusions, and polypoid endobronchial tuberculous lesions, which may be responsible for atelectasis, can all be identified with CT.249.250.251. and 252. The presence of hilar or mediastinal lymphadenopathy is readily confirmed or detected. 246 The lymph nodes in tuberculous lymphadenitis, particularly when over 2 cm in diameter, show a low-density center with rim enhancement of the periphery.246.253. and 254. CT demonstrates that subcarinal lymphadenopathy is almost invariably present (but very rarely confined to this region), and this accounts for the relative frequency of compression of the mainstem bronchi. 254 Primary tuberculosis may be complicated by tuberculous meningitis or miliary tuberculosis (Fig. 5.54), both conditions of the utmost seriousness. Miliary tuberculosis may be detected by HRCT at a stage when the chest radiograph may be normal.246. and 255.
Pulmonary tuberculosis associated with AIDS and other immunosuppressed states, such as myelodysplastic syndromes, 256 has many of the clinical and radiographic features of primary tuberculosis even when there is strong evidence that the disease represents reactivation of previously acquired infection. In this situation the hypersensitivity reaction appears to be in abeyance and caseous necrosis is much less frequent, and it seems that the clinical and imaging features are related to the patient’s CD4 lymphocyte count. 257 Generally speaking, with CD4 lymphocyte counts above 200/mm3 the radiographic features are those of usual reactivation tuberculosis. With CD4 lymphocyte counts falling below 200/mm3 the findings increasingly resemble primary tuberculosis albeit often more severe than usual. Thus hilar and mediastinal adenopathy is very frequent while cavitation is much less common.258.259.260.261. and 262. Consolidation may be seen in any part of the lung and dissemination in the form of miliary tuberculosis, tuberculous bronchopneumonia and tuberculous pleurisy has a higher frequency with low CD4 lymphocyte counts. On the other hand Greenberg et al. 263 found normal chest radiographs in 21% of AIDS patients with proven tuberculosis and CD4 lymphocyte counts of less than 200/mm3. Furthermore in the 133 patients in this series, one-third had no chest radiographic findings suggestive of primary, reactivation or miliary tuberculosis. Patients with AIDS are more likely to be sputum-positive for M. tuberculosis and have a greater tendency to extrathoracic dissemination. 264 The subject is discussed at greater length in Chapter 6.
Reactivation (postprimary) tuberculosis
Focal pulmonary tuberculosis
In the earlier phases reactivation tuberculosis gives rise to patchy subsegmental consolidations with ill-defined margins (Fig. 5.55) and a tendency to coalesce so that there may be small satellite foci in the adjacent lung. There is a predilection for the posterior aspects of the upper lobes and the superior segments of the lower lobes (Fig. 5.56), although no portion of the lungs is immune. 265 For example, predominant or exclusive involvement of the anterior segments of the upper lobes has been described in a small percentage of patients (Fig. 5.57). 266 Anecdotally, focal tuberculosis in unusual locations is more frequent in patients with a background of diffuse pulmonary fibrosis, and in this setting the masslike disease may be interpreted as representing a pulmonary neoplasm. Bilateral and multilobar involvement is fairly frequent. The consolidations are usually peripheral in location, and therefore conspicuous air bronchograms are not present. Some focal pleural thickening may be present in the early stages even in the absence of pleural effusions (Fig. 5.58).
Cavitation is a distinct feature of reactivation tuberculosis and is a finding of considerable diagnostic importance, since it usually indicates disease activity (Fig. 5.59). Even quite small pulmonary foci may cavitate, and multiple cavities of varying size may be present. Fluid levels may be seen (Fig. 5.59) and may aid in the recognition of cavities, the walls of which may be indistinct or obscured by overlying densities. Frequently, however, fluid levels are not present. Apical bullae if present may be misinterpreted as cavitation, a mistake that can often be avoided if it is borne in mind that cavities are centered within areas of consolidation and do not merely overlap them. Patients with cavitary disease represent a potential threat to those who come into contact with them, and therefore immediate measures to prevent the spread of disease may be appropriate on the basis of the radiographic findings alone.
Widespread bronchopneumonia presumably results from a breakdown in host defenses with spread of disease via the airways. It is usually patchy and bilateral and may involve portions of lung less commonly affected by tuberculosis, such as the middle lobe or the anterior segments of the upper lobes. Fibrocalcific changes may be seen elsewhere in the lungs if the bronchopneumonia stems from breakdown of preexisting chronic fibrocaseous tuberculosis.
In immunocompromised hosts tuberculous bronchopneumonia may become extensive and may be fatal. Cavitation may not be present in the early phases even when the patient has extensive, patchy confluent perihilar consolidation.
Endobronchial tuberculosis
Endobronchial tuberculosis is difficult to diagnose simply because involvement of the airways is not readily evident on chest radiography. 267 This is one reason why the incidence of endobronchial tuberculosis is uncertain, but it is thought to occur in 10–40% of individuals with active pulmonary tuberculosis. 268 Tuberculous granulomatous cicatrization may cause a bronchial stricture, which in turn may cause obstructive atelectasis. 269 The associated pulmonary parenchymal lesions may be obscured by the atelectasis (Fig. 5.62). CT is key for the detection of endobronchial disease and the planning of interventional treatment such as balloon dilatation of a stricture.270. and 271.
Broncholiths represent a late complication of pulmonary tuberculosis and histoplasmosis (Fig. 5.63).272. and 273. A calcified lymph node may erode into an adjacent airway and be associated with hemoptysis or pneumonia. A broncholith in one of the segmental bronchi is easy to overlook because calcifications at hilar level are assumed to be in lymph nodes outside the bronchial lumen. Rarely a patient reports recurrent lithoptysis and serial radiographs show a large central calcified node disappearing as material is discharged into the bronchus and expectorated. Broncholithiasis is discussed more fully in Chapter 12.
Tuberculomas are discrete tumorlike foci of tuberculosis in which there is a fine balance between activity and repair. The margins of tuberculomas are usually well circumscribed (Fig. 5.64), although some irregularity or focal loss of definition may occur because of adjacent fibrous changes. Tuberculomas may be multiple and on occasion become large, up to 5 cm in diameter. Some growth may be perceptible over an extended period of observation. Calcification develops in the central caseous core with time and it is often detectable radiographically. It may be amorphous, and if the core is large in relation to the cellular mantle, a nodule of uniform increased density will result, whereas with a more confined central core of calcification a line of demarcation may be apparent (Fig. 5.65). Calcifications that are more laminar, flecklike, or punctate also occur and are easier to appreciate because variable density is noted within the nodule. Tuberculomas show little tendency to break down, and cavitation is rare. Cavitation strongly suggests reactivation. In general, the overlap in imaging features between a tuberculoma and lung neoplasm is such that the distinction cannot be made on the basis of CT features alone (as an aside both diseases may very rarely be present in the same lesion). 274 On positron emission tomography (PET) the majority of tuberculomas show increased [18 F]2-fluoro-2-deoxy-d-glucose (FDG) update and so may be confused with a pulmonary neoplasm. 275
Miliary tuberculosis, which results from hematogenous dissemination of the disease, is an infrequent but feared complication of both primary and reactivation tuberculosis. As with other forms of reactivation tuberculosis, the miliary form may be the consequence of a degree of immunosuppression, for example a patient with rheumatoid arthritis treated with infliximab. 276 The lungs show a myriad of 2–3 mm granulomatous foci whimsically likened to millet seeds (hence miliary) in size and appearance. The radiographic result is widespread fine nodules, which are uniformly distributed and equal in size (Fig. 5.66). Because there is a threshold below which the nodules are invisible, miliary tuberculosis can be present in patients with a normal chest radiograph. Kwong et al. 277 in a retrospective review of 71 patients with miliary tuberculosis found approximately a third of chest radiographs at the time of diagnosis were considered normal. On or near the threshold of visibility the nodules may appear and disappear on serial radiographs. Miliary nodules are more readily detected with HRCT (in 24/25 cases in one series) 278 and have a random distribution in relation to the secondary pulmonary lobule255. and 279. (Fig. 5.67); there are often patches of ground-glass opacification superimposed on the miliary pattern, and when these areas are extensive they may herald the development of ARDS. 278 Miliary tuberculosis does not leave residual calcifications. Miliary nodulation of the lung has numerous causes other than tuberculosis (see page 141), but tuberculosis is the preeminent consideration because prompt diagnosis and treatment are vital.
Any tuberculous focus may involve the adjacent pleura, and some degree of focal pleural reaction and thickening is relatively common. Im and associates283 studied apical tuberculosis with HRCT and made the interesting observation that the apical pleural thickening commonly seen with fibrocaseous tuberculosis is composed largely of extrapleural fat. The fat can be considered a packing material that fills space as the underlying lung undergoes fibrous contraction. Pleural effusions are not uncommon in patients with widespread tuberculosis. Tuberculous pleuritis, which may occur in the absence of a radiographically visible pulmonary focus, must be considered in the differential diagnosis of any large unilateral pleural effusion for which no adequate cause can be established radiographically, clinically, or by pleural fluid analysis (Fig. 5.69). Less commonly the pleural reaction is more cellular, resulting in diffuse irregular pleural thickening resembling pleural metastatic disease or mesothelioma. 284 CT may demonstrate a pulmonary focus that is not visible on the chest radiograph. In one series 86% of patients with tuberculous pleuritis had lung lesions on CT and about two-thirds of the study group were considered to have active pulmonary tuberculosis. 285 Frequently, the diagnosis of tuberculous pleuritis can only be established by pleural biopsy.
The response of tuberculous pleurisy to appropriate treatment is varied. All traces of pleural reaction may clear, but it is common to see residual pleural scarring with obliteration of the costophrenic sulcus and distortion of the diaphragm. It has been reported that a rapid rate of reduction in volume of pleural fluid, after 2 weeks of appropriate drug treatment, is the best predictor of the degree of residual pleural scarring. Residual thickening may be severe, and particularly in these cases the lung can become restricted by the encompassing fibrous tissue and calcification.
Tuberculous pleurisy may become localized and form a tuberculous empyema (Fig. 5.70). 286 The empyema may break through the parietal pleura to form a subcutaneous abscess, the so-called empyema necessitatis. The empyema cavity may also be connected to the bronchial tree by a fistulous track (Fig. 5.71). Drainage of such lesions may result in a chronic bronchopleural fistula that can be extremely resistant to treatment. CT is useful in delineating foci of activity in pleural tuberculosis evidenced by fluid collections within the rind of pleural thickening. Tuberculosis was at one time a common cause of spontaneous pneumothorax, although today this complication is rare.
Some of the most remarkable radiographs result from various forms of collapse therapy dating from preantibiotic time, but survivors from this era are diminishing. The thoracoplasty involved resecting a varied number of ribs to collapse the chest wall onto the underlying lung (Fig. 5.72). In many instances only a small portion of the lung at the base remains aerated and the majority of the lung is obliterated. There is almost inevitably some residual fibrocalcific thickening underlying the thoracoplasty. Various other materials or objects were inserted extrapleurally to compress the underlying lung. These included paraffin, mineral oil, and Lucite balls (Fig. 5.73). 287 Collapse therapy with pneumothoraces always produced some pleural thickening.
Chest radiography plays a vital role in the detection and control of pulmonary tuberculosis. Serial radiography is important in gauging the activity of lesions and their response to treatment. It is hazardous to estimate activity on the basis of a single radiographic examination; even though fibrous infiltration and calcification may be prominent features, active foci may be present. Tuberculous foci that appear inactive over an extended period of observation may contain viable organisms with the potential to break down under adverse circumstances. Miliary nodulation definitely indicates activity, and cavitation is a strong indication of active disease. In practice, the physician is often obliged to base certain judgments on the findings of a single radiographic examination. For example, isolation and aggressive investigation may be urged for one patient, whereas another may be allowed to proceed to routine surgery when seemingly ‘inactive’ fibrocalcific apical scarring is present. Nevertheless, the physician cannot afford to be too cavalier about the latter type of case, and some additional study such as comparison with a previous film or a follow-up examination is usually advisable.
CT of pulmonary tuberculosis
The CT findings in the various forms of tuberculosis have been established in a series of papers on the subject.249.250.252.255.283.288.289.290.291.292.293.294.295. and 296. Some of the indications for CT and the findings are reviewed in the following paragraphs.
The presence of cavities strongly suggests that the disease process is active, particularly if the outer margins of the cavitary process are ill defined and there are satellite centrilobular ‘rosettes’ of infiltrates in adjacent lung (Fig. 5.74, Fig. 5.75 and Fig. 5.76). The inner wall of a tuberculous cavity is smooth or irregular, and the cavities usually contain only a small amount (if any) of fluid. In one series of patients with early tuberculosis, cavities were detected in 58% of the initial CT studies, whereas the corresponding figure for the radiographs was only 22%. 288 The CT detection of a cavitary process underlying and obscured by a large pleural effusion may be an important pointer to the diagnosis of tuberculous pleurisy. There may be an increased frequency of cavitation (and also unusual localization of disease) in diabetic and immunocompromised patients. 297
CT detects infiltrates not seen on radiographs and can help to explain the presence of hilar or mediastinal adenopathy, particularly in adult patients. The quality and pattern of pulmonary nodules is quite variable (Figs 5.75 and 5.76). The nodes themselves may show the characteristic features of central low density and rim enhancement.290. and 291. At a later stage, calcification may be detected. In a series of over 40 children with tuberculosis, Kim et al. 246 found that, in 20% of cases, the diagnosis was suggested only on the CT scans. The findings included nodules of bronchogenic spread and miliary infiltration not detected on plain radiographs. CT is more sensitive than chest radiographs in the detection of miliary tuberculosis.
Although hemoptysis is a classic symptom of tuberculosis, more profuse hemoptysis or recurrent hemoptysis may require additional imaging studies such as angiography or CT. Generally, tuberculosis patients with hemoptysis have disease of some chronicity with major structural changes. Fungus balls within a chronic tuberculous cavity may be associated with semi-invasive aspergillosis – such fungus balls may not always be detectable on chest radiography. 298 Reference has already been made to the use of CT in the detection of broncholithiasis. Bronchiectasis in association with tuberculosis is readily detected by CT. 299
Complications include empyema, 286 extension of infection through the chest wall (empyema necessitatis), bronchopleural fistula formation, fibrosing mediastinitis, 295 endobronchial tuberculosis leading to strictures, occlusions and fistulae, 300 pericarditis and constrictive pericarditis, and esophagomediastinal fistulas resulting from nodal erosion into the esophagus.269. and 301. The various intrathoracic complications are summarized in Box 5.8.
• Esophageal tuberculosis secondary to active pulmonary disease – ulceration, strictures, fistulas, diverticulum formation
• Spine and chest wall involvement by hematogenous or direct spread – Pott disease, empyema necessitatis, osteitis of ribs
• Secondary pyogenic infections in chronic disease
• Associated chest diseases
– Silicosis – increases susceptibility to tuberculosis
– Lung cancer – may be associated with reactivation of tuberculosis
In terms of assessing the activity of tuberculosis, a word of caution is necessary: seemingly inactive thin-walled cavities with associated fibrous infiltrates and calcification may be associated with the presence of tubercle bacilli in the sputum. Nevertheless, there are CT features highly suggestive of activity; these features are summarized in Table 5.1. Cavitation, particularly if extensive and irregular with a thick wall or in an area of consolidation, is highly suspicious. However, adjacent areas of lung should be studied with care as there may be important associated findings. These include nodulation resulting in branching opacities, tree-in-bud appearance, ground-glass opacity, and centrilobular rosettes of infiltration. Not surprisingly patients with a positive sputum smear have a higher frequency of these signs of exudative disease than smear-negative patients.302.303.304. and 305. Miliary infiltration of the lungs is an absolute indicator of activity. The association of pleural and pericardial effusions with parenchymal changes of tuberculosis is a strong indicator. In the hilum and mediastinum, activity is indicated by lymph nodes showing central low density with rim enhancement. Tracheobronchial changes indicative of activity include irregular wall thickening with narrowing or obstruction, contrast enhancement of the thickened wall and peripheral peribronchial cuffing indicative of peripheral spread of disease. Features which indicate previous tuberculosis but do not in themselves indicate activity are also given in Table 5.1. It should be noted that certain features such as calcification, cavity formation, and pleural thickening appear in both columns in Table 5.1.
Many mycobacteria other than M. tuberculosis have been identified as causes of pulmonary infection. Mycobacteria are common in the natural environment, and numerous species exist.306. and 307. The term ‘environmental opportunistic mycobacteria’ has been proposed in preference to nontuberculous, or atypical, mycobacteria (because pedantically these organisms are capable of causing tuberculous lesions); 306 another somewhat cumbersome term ‘mycobacterium other than tuberculosis’ (MOTT) has also been used, 308 but in what follows the widely used term nontuberculous mycobacteria (NTM) will be used. The NTM species capable of causing pulmonary infection include, in approximate order of incidence: M. avium–intracellulare, M. kansasii, M. abscessus, M. xenopi, M. fortuitum-chelonae, M. malmoense, M. gordonae, M. szulgai, M. simae, M. scrofulaceum, and M. genavense.309.310. and 311. The incidence of NTM disease in the immunocompetent population is between 0.5 and 10 cases per 100000 population, an incidence of approximately one-fifth that of tuberculosis, although the proportion of nontuberculous mycobacterial infections is probably rising. 311 The incidence has remained fairly stable possibly because infection occurs from the natural environment (sources are water, soil, and dust) and not by person-to-person transmission.
• Nontuberculous mycobacteria (NTM) are omnipresent in the environment, particularly in water and soil, with wide geographical variations in prevalence of nontuberculous mycobacterial species
• The range of species and incidence of important NTM pulmonary infection continues to rise
• As well as differences between the NTM species, differences in host defense may modify the manifestations of NTM disease
Classification
• NTM species can be broadly divided into fast- and slow-growing types
• The commonest and most important slow-growing species is M. avium–intracellulare (MAC) (increasing incidence worldwide)
• Sophisticated nucleic acid profile analysis of NTM may aid species-specific diagnosis
Clinical presentation
• The level of host immunity has a profound effect on the severity of infection caused by NTM
• The slow-growing NTM (e.g. MAC) cause a subtle and variable granulomatous response once the bronchial mucosa surface is breeched
• A secure diagnosis of pulmonary NTM infection can be made only when microbiologic, clinical and imaging findings are all taken into account
• A normal chest radiograph does not preclude the diagnosis of nontuberculous mycobacterial infection
The mechanisms by which these common organisms cause progressive and potentially fatal disease in some individuals but not others are ill understood but probably relate to a cryptic deficiency in the host’s immunocompetence. One of the problems in the study of the clinical and imaging manifestations and epidemiology of NTM infections has been that these organisms may occur as incidental contaminants. Over 100 species of NTM have now been identified312 and with more sophisticated techniques for ‘typing’ these organisms, making a definitive classification is elusive. 313 Historically, NTM have been divided into fast- and slow-growing (on culture) types, M. avium–intracellulare complex (MAC) being the most important of the slow-growing NTM. Because NTM are ubiquitous, respiratory secretions often contain these organisms, and these can be detected by extremely sensitive polymerase chain reaction tests; however, such detection does not necessarily indicate clinically important pulmonary infection and the distinction between ‘colonization versus infection’ is an important one addressed in guidelines from the American Thoracic Society. 314 The three fundamental requirements, simplified here, needed to make a diagnosis of NTM pulmonary infection are: (1) the time course and clinical presentation must be compatible; (2) the radiographic findings (including a normal chest radiograph) must be consistent; and (3) the NTM organism must be recovered in sufficient numbers from either sputum or bronchial washings. 314 In summary, synthesis of all available information is needed to make a secure diagnosis of NTM pulmonary infection.
Immunocompetent patients infected by NTM can be broadly divided into two groups. One comprises patients, usually older men, with preexisting lung disease, such as chronic obstructive airways disease, fibrosis as a consequence of healed tuberculosis, or fungal infections, bronchiectasis and cystic fibrosis. 315 Another distinctive group comprises predominantly elderly women with no obvious preexisting pulmonary or systemic disease.316. and 317. Immunocompromised patients, particularly those with AIDS311.318. and 319. or following lung transplantation, 320 have an increased susceptibility to NTM infection. Compared with tuberculosis, NTM pulmonary disease is relatively indolent and runs a chronic course, sometimes remaining static for months, or indeed years: radiographic abnormalities attributable to NTM have been reported to remain stable for up to 12 years. 321 However, without treatment NTM pulmonary infections may progress in some individuals and may ultimately be fatal321 (Fig. 5.77).
A broad spectrum of radiographic appearances has been attributed to NTM infections; a common theme in many studies to date is the lack of imaging differences between NTM and conventional tuberculosis. Table 5.2 indicates the considerable overlap in imaging findings between tuberculosis and NTM infection, and indeed between the NTM species.
However, there are radiographic features that, although not diagnostic, raise the possibility of an NTM infection, and very occasionally provide clues as to the specific species of NTM organism responsible. The radiographic features may be modulated by the type of patient infected. Those with preexisting pulmonary disease, typically elderly men, tend to have upper lobe cavitary disease (Fig. 5.78) as described by Christensen and colleagues322 in their review of M. kansasii infections. This has been termed the ‘classical’ appearance323 and is very similar to conventional pulmonary tuberculosis324 (Fig. 5.79). Clinically these patients have constitutional symptoms including weight loss, fever, malaise, cough, and hemoptysis.310.325. and 326. A bias towards the reporting of cavitary disease, hence this ‘classical’ appearance, results from the use of sputum culture to confirm diagnosis.325. and 327. With the advent of more invasive diagnostic techniques such as bronchoscopic washings328 and lung biopsy, which yield positive results despite a lower burden of mycobacterial organisms, a picture less reminiscent of typical tuberculosis has emerged. 323 This pattern is typically found in elderly women with no underlying pulmonary disease; 329 the picture is characterized by multiple nodular opacities, bronchiectasis, and focal consolidation. 330 Constitutional symptoms are absent or mild in these patients. 325
The radiographic appearances of the majority of NTM pulmonary infections in immunocompetent patients will reside within the spectrum of predominantly cavitary through to predominantly bronchiectatic/nodular pattern. The latter (less destructive) pattern may progress to the cavitary pattern. However, variations occur and some patients, such as patients with cystic fibrosis,331. and 332. and patients subject to repeated aspiration, such as those with esophageal achalasia or gastric outlet obstruction, have a predisposition for NTM infections;333. and 334. in these patients the radiographic appearances may be large areas of confluent consolidation (Fig. 5.80), quite unlike the less florid appearances of MAC infection (see below). Very rarely NTM infection may present as a focal pulmonary mass with CT features suspicious of malignancy. 321 Nevertheless, these can be regarded as very unusual presentations of NTM infection. Localized pleural reactions occur, but pleural effusions are uncommon. Adenopathy and miliary spread of disease are excessively rare.
Bronchiectasis is a very frequent accompaniment to NTM infection, particularly with MAC. 335 Longitudinal CT studies of patients infected with MAC have shown progression of bronchiectasis in some, suggesting MAC infection as a primary cause of bronchiectasis rather than merely an opportunistic infection of deranged airways.326. and 336. Cavitation is seen in both conventional tuberculosis and NTM infections and various studies have compared the characteristics of cavitation on chest radiography in an attempt, perhaps over-optimistically, to differentiate between the two. There are conflicting reports about the size and wall thickness of NTM versus tuberculous cavities.322.324.325.327. and 336. The reported discrepancies probably reflect the varying stages of disease, and the characteristics of cavities, and particularly cavity wall thickness, do not allow discrimination between MAC infection and conventional tuberculosis in individual cases.
There is an increasing number of reports on the imaging of individual NTM species and these are summarized below.
Mycobacterium avium–intracellulare complex
In clinical practice pulmonary infection by MAC is frequently overlooked, partly because the symptoms and signs are so nonspecific. 337 The manifestations of MAC are modulated by the immune status of the host and the presence or absence of preexisting lung disease, thus the spectrum can range from a few inconspicuous nodules through to destructive cavitating disease on a background of emphysema. Descriptions in the past have categorized the pattern of pulmonary disease caused by MAC as either classic or nonclassic in appearance;309. and 323. this distinction alludes to the occasional similarity between the appearances of MAC infection and the ‘classic’ picture of conventional reactivation tuberculosis. However, a clear resemblance to one or other of these two nominal forms is often absent and the value of making this arbitrary distinction is questionable. Chest radiography has a valuable role in monitoring patients with a confirmed diagnosis of MAC, whereas HRCT, which shows the sometimes subtle morphologic abnormalities caused by MAC infection, can detect earlier disease and suggest the diagnosis.
The less florid form of MAC infection, now more frequently recognized than the ‘classical’ form, is seen most often in elderly women with no obvious preexisting lung disease or clearly characterized immune defect. In such individuals, the radiographic manifestations of MAC infection range from normal appearances, through small inconspicuous nodules (ranging from a few millimeters to approximately 1.5 cm) to foci of consolidation and signs suggestive of bronchiectasis. The exact nature of the nodules depicted on chest radiographs is not always clear, but those at the smaller end of the spectrum probably correspond to exudate in and around small airways, reflecting endobronchial spread (and likely corresponding to the HRCT finding of a tree-in-bud pattern). Although there are few longitudinal radiographic studies of the natural and treated history of MAC infection, there does not appear to be an inevitable progression of what can be regarded as relatively minor abnormalities (nodular disease, bronchiectasis) to more advanced and destructive disease (cavitation and fibrosis). Indeed, the relatively indolent disease usually associated with elderly women may wax and wane without treatment, such that some nodules may disappear spontaneously (Fig. 5.81), only to reappear at different locations months or years later. In the series of Woodring et al., 338 the average time over which there was definite radiographic progression in patients with MAC infection was 6.4 years. In the same study the authors remark on the delay, anywhere between 1 and 16 years, between presentation and the diagnosis of MAC – again highlighting the nonspecific nature of the clinical and radiographic findings. 338 An uncommon manifestation of MAC is as a single focal pulmonary mass or solitary nodule on plain chest radiograph. 339
There are no clear distribution characteristics of the radiographic abnormalities of MAC infection. Nevertheless, bronchiectatic changes in the right middle lobe and lingula (Fig. 5.82) may be particularly prominent in some elderly women with the nonclassic form of disease and the term ‘Lady Windermere syndrome’ has been coined for this pattern. 340 Given that bronchiectasis of other causes or association may be concentrated in these lobes, this characteristic alone cannot be taken as having a high predictive value for MAC infection, and some take exception to the name Lady Windermere syndrome. 341
The typical constellation of HRCT features of MAC infection (Box 5.10) are bronchiectasis (may be predominantly in the right middle lobe and lingula), centrilobular nodules (usually a tree-in-bud pattern), a few scattered larger nodules approximately 1 cm in diameter (one or two of which may show cavitation) and a few small foci of consolidation (Fig. 5.83).317.327.328.330.342.343. and 344. Although these individual abnormalities are nonspecific, the combination, particularly in an elderly woman, is very suggestive of MAC, and the radiologist is in a position to be the first to raise the possibility of MAC infection. Marked cavitation is a less frequent manifestation of MAC (Fig. 5.84) infection compared with conventional tuberculosis. 342 When present, cavitation is associated with an increased incidence of positive sputum smears and culture.327. and 345. Compared with other NTM species, bronchiectasis in patients with MAC tends to be more extensive and severe. 335
The predictive value of HRCT for the diagnosis of significant MAC infection has been reported in several studies. Tanaka et al. 328 followed 26 patients with HRCT appearances suggestive of MAC infection for 4 years. Half of these individuals subsequently proved to be culture positive for MAC (from sputum samples or from bronchial washings). Similarly, a study by Swensen et al., 317 using the criterion of bronchiectasis with coexistent nodules in the same lobe, found that just over 50% of individuals had culture-positive MAC (as opposed to 4% of individuals with CT evidence of bronchiectasis but no lung nodules), suggesting a relatively high specificity of 87% and a sensitivity of 80%. A more recent study reported a lower prevalence (17%) of MAC in patients with bilateral bronchiectasis and ‘bronchiolitis’ (tree-in-bud pattern). 344
In a further study by Hartman et al. 330 the combination of bronchiectasis and nodules in the same lobe, particularly when the middle lobe/lingula were the predominant sites of involvement, was highly suggestive of MAC infection. While the pathologic correlate of the tree-in-bud pattern in the context of MAC infection is likely to represent exudate in and around the small airways, the nature of the randomly scattered nodules is less certain. The irregular shape and nontubular nature of these randomly scattered opacities makes mucus impaction an unlikely explanation; some of these nodules contain air bronchograms, suggesting that they represent foci of infective consolidation. Occasional cavitation is seen in nodules and a longitudinal CT study has suggested that the connection between a terminal or lobular bronchus and the cavity, identifiable on CT, indicates that this is where the infective nidus takes hold and develops. 346 The nodules, with or without cavitation, sometimes abut the pleural surface and this may be the reason why occasional pleural effusions or localized pleural thickening are seen on CT. 346
In addition to the cardinal features of bronchiectasis and exudative small airways involvement (tree-in-bud pattern), HRCT sometimes reveals a mosaic attenuation pattern reflecting obliterative small airways disease (Fig. 5.85). Whether this is associated with preexisting bronchiectasis, or a direct consequence of MAC infection, as suggested by Kubo et al., 347 is unclear.
The radiographic appearances of M. kansasii infection tend to resemble those of conventional tuberculosis. 324 Infections are almost always cavitary involving the upper lobes with coexisting fibrotic destruction and opacities. Cavities found in M. kansasii varied widely in size and wall characteristics (Fig. 5.86) offering no distinguishing features when compared with those of tuberculosis.322. and 348.M. kansasii is, unlike other NTM infections, responsive to conventional antituberculous drugs and is particularly prevalent in middle-aged men with predisposing factors such as alcohol misuse, COPD, 349 or previous mycobacterial or other debilitating diseases. 350
M. xenopi infections have very similar radiographic appearances to M. kansasii. The upper lobes are usually involved with cavitation and fibrosis and no characteristic appearances have been reported (Fig. 5.87). 351 In one series, bronchiectasis was present in all cases335 but totally absent in another. 351 The imaging description of M. abscessus352 adds yet another mycobacterial species that has relatively nonspecific features, in this case small nodular opacities, bronchiectasis, and cavity formation. 353
A comparative study suggested that cavities larger than 6 cm, and air–fluid levels within cavities, favor M. malmoense infection, 354 but the previously mentioned reservation about applying this observed trend to an individual case applies. There is an important report of coexisting chronic necrotizing aspergillosis in some patients with M. malmoense infection; 355 the possibility of these two low-grade infections (that is, aspergillosis with any species of NTM) coexisting in elderly or debilitated patients is always worth considering356 (Fig. 5.88). Mycobacterium chelonae has a pattern of disease similar to that of MAC with frequent bronchiectasis and nodules, although cavity formation was more common than in MAC.352.353. and 357. In one series, M. chelonae and M. fortuitum were more frequent in younger patients (i.e. compared with the older age range usually associated with MAC); 335 and these two species, and the increasingly recognized M. abscessus, seem to be relatively frequent pathogens in patients with cystic fibrosis.358. and 359. These fast-growing NTM are important because they are relatively resistant to drug treatment. 360
In a study of 19 patients with M. gordonae infection the authors concluded that there were no characteristic radiographic findings associated with M. gordonae infections and that in each case studied there was an alternative differential diagnosis for the radiographic findings, such as community-acquired pneumonia, tuberculosis, or carcinoma. 361M. gordonae is usually a nonpathogenic colonizing organism.
Most cases of pulmonary nocardiosis are due to Nocardia asteroides, although other Nocardia species, notably Nocardia brasiliensis, are occasionally implicated. Nocardia is a filamentous, Gram-positive, weakly acid-fast bacillus that grows very slowly on aerobic cultures. It has similarities to Actinomyces362 and although Nocardia infections occur worldwide, they are relatively rare in immunocompetent individuals. Nocardiosis is seen particularly in patients on immunosuppressive therapy363 and those who have received organ transplants364 and in individuals with chronic illness, especially HIV, 365 other underlying immunologic deficiency, or alveolar proteinosis. 366 Obstructive lung disease, particularly cystic fibrosis, seems to predispose to Nocardia infection.367. and 368. A variable proportion of patients have no recognizable underlying condition. 369 The incidence of nocardiosis appears to be increasing, probably because of the increasing prevalence of immunocompromised patients. Dissemination from the lungs to other organs, notably the brain, may occur (in a quarter of patients in one series of patients with chronic granulomatous disease). 370 In the lung, Nocardia typically causes single or multiple chronic cavitating lesions similar to the lesions caused by pyogenic bacteria or indeed tuberculosis. 371 Fibrosis is a late development, and pleural involvement, usually either fibrous thickening or empyema, is frequent.
• CT may show central low attenuation cavitation and more nodules
• Focal nonspecific consolidation or infiltrates – much less common
• Pleural involvement frequent – effusion or empyema
The chest radiographic findings are variable.372. and 373. Pulmonary consolidation is the most common feature. The consolidations are usually large and frequently cavitate (Fig. 5.89). They may be unifocal or multifocal and may be patchy, segmental, or occasionally lobar. Some patients have single or multiple round pneumonias (Fig. 5.90), which can be irregular and may cavitate, giving rise to a thick-walled abscess. In such cases the distinction from bronchial carcinoma may be difficult. 374 Similarly the rare endobronchial mass caused by nocardiosis may exactly mimic a tumor radiographically and at bronchoscopy. 375 Rarely, diffuse consolidation or widespread reticulonodular shadows are encountered. Pleural effusions that may lead to empyema, and hilar and mediastinal adenopathy, are reported features of the disease. Nocardia can occasionally form a fungus ball similar to an aspergilloma, 376 and a nocardial mass in the anterior mediastinum of a patient with sarcoidosis has been reported. 377
The dominant CT findings are focal nodules or masses or focal areas of consolidation showing central low attenuation, with or without cavitation378. and 379. (Fig. 5.91). Extension to the pleura or even the chest wall occurs resulting in pleural fluid, pleural thickening, or empyema.
• A. israelii – a filamentous, anaerobic Gram-positive bacillus
Route of infection
• Infection of devitalized or infected tissues mainly of the jaw, gastrointestinal tract or the lung. Patients are often alcoholics with poor dental hygiene but otherwise not immunocompromised
Radiology
• A suppurative pneumonia causing consolidation or a masslike lesion
• Cavitation common
• Spread to the pleura (empyema) or the chest wall (rib destruction or periostitis, soft tissue mass, fistula) is characteristic
• Lymphadenopathy is common
• Mediastinal/spinal invasion can occur
The chest radiograph384.385. and 386. and CT387.388. and 389. usually reveal an area of persistent subsegmental consolidation (Fig. 5.92) or a mass (Fig. 5.93), either of which may cavitate. The similarity to bronchogenic carcinoma390 or tuberculosis391. and 392. frequently leads to diagnostic confusion. Indeed the diagnosis may only be made following surgical reflection of a presumed neoplasm393. and 394. (Fig. 5.94). As with nocardiosis, actinomycosis may cause an endobronchial mass that may be confused with bronchial carcinoma at bronchoscopy;395. and 396. furthermore actinomycosis may be associated with broncholithiasis.381. and 389. Focal fibrosis and contraction may be striking. Widespread small nodular shadowing has been reported. 395 The infection readily transgresses the pleura and therefore crosses fissures and extends into the chest wall, but this is now a less common manifestation possibly because of effective antibiotic therapy.384. and 396. It is important to recognize that Actinomyces will colonize devitalized tissue, and that damaged lung (preexisting scarring or bronchiectasis) is prone to this infection; 397 thus the presence of localized bronchiectasis within, or adjacent to, masslike consolidation may point toward the diagnosis of actinomycosis (Fig. 5.95).
Pleural involvement is manifest as pleural effusion, pleural thickening, or empyema formation but is seldom associated with large accumulations of fluid. Pleural thickening was found at CT in all eight cases reported by Kwong and co-workers; 387 the pleural thickening was smooth and localized to the pleura abutting the diseased lung. Rib involvement leads to lysis and visible periostitis, which is readily seen with CT (Fig. 5.96). Similarly, if the spine is involved, there may be a lytic lesion in the spine adjacent to the pulmonary or pleural shadowing.387. and 398. Mediastinal invasion with pericardial and cardiac involvement has been reported,383.397. and 399. but this is rare. CT demonstrates chest wall (Figs 5.94 and 5.96) 400 pleural,387. and 388. mediastinal (Fig. 5.95), and spinal invasion to advantage; 383 it also demonstrates intrathoracic lymphadenopathy, up to 2.5 cm in diameter, in a high proportion of patients.387. and 400.
Botryomycosis is a very rare chronic infectious disease that resembles actinomycosis both clinically and pathologically, in that gray–yellow granules similar to the sulfur granules of actinomycosis are a feature of the infection. 396 Reports are scant but, as with actinomycosis, patients may present with masslike, cavitating, or endobronchial lesions that resemble a bronchogenic carcinoma (Fig. 5.97) whereas, in others, the lesions involve the pleural space.401.402.403. and 404. This unusual infection may be localized distal to an endobronchial foreign body. 404
Fungi include mushrooms, molds, and yeasts, but few of these organisms consistently cause pneumonia in humans.405. and 406. A mold is a microscopic, multibranched tubular structure that grows at its expanding margin by the elongation of hyphal tips and by producing new branches, known as hyphae. The yeast shape is another morphologic form taken by some fungi. Yeasts are single, ovoid to spherical cells with rigid walls, in which multiplication occurs by the development of buds, with the cytoplasm and at least one nucleus moving into the bud. The distinction between certain bacteria and fungi is not clear, and some pathogenic organisms such as Nocardia and Actinomyces, originally thought of as fungi, are considered to be bacteria. Pneumonias caused by Candida, Aspergillus, and Mucor are predominantly seen in immunocompromised patients and are discussed on pages 322–330. The following section discusses the agents responsible for most fungal pulmonary diseases that usually occur in endemic areas, 407 namely histoplasmosis, cryptococcosis, coccidioidomycosis, North American blastomycosis and aspergillosis, and then briefly describes sporotrichosis and geotrichosis. Although some fungal diseases may resemble tuberculosis in their manifestations, they show a wide variety of radiographic patterns and indeed may closely resemble an endobronchial lung cancer. 408
• Massive airway inoculation leading to diffuse bronchopulmonary disease
Acute disseminated form
• Hematogenous dissemination to liver, central nervous system, lungs, bone marrow, adrenals, etc. Rare, more common in immunocompromised patients
Pulmonary histoplasmosis
• Fleeting focal pneumonitis with hilar and mediastinal adenopathy
• Few if any symptoms. Self-limiting. Very common in endemic areas
• Histoplasmoma formation – single or multiple nodules with or without calcification
• Chronic cavitary histoplasmosis. Uncommon. Middle-aged to elderly men living in a rural environment in an endemic area. COPD is a predisposing factor
Mediastinal histoplasmosis
• Mediastinal adenopathy common
• May involve the mid-esophagus – dysphagia, diverticulum formation
• Can extend to involve the pericardium – pericarditis, constrictive pericarditis
• Fibrosing mediastinitis – commonest cause in the USA. Causes obstruction of the superior vena cava, major bronchi, or major central pulmonary vessels
Liver and spleen granulomata
• Common. A mild innocuous form of dissemination
Bone involvement
• Rare with H. capsulatum but common with H. gondii in Africa
Most human infection results from inhalation of airborne spores that germinate and convert to the yeast form. Dissemination then occurs via the blood and lymphatics. In immunocompetent individuals the fungus multiplies intracellularly until cell-mediated immunity has developed. Macrophages can kill the fungus and this produces intense inflammation. Caseous necrosis occurs, followed by calcification. In infants, as well as in patients with reduced T cell mediated immunity (such as those who are taking steroids or immunosuppressive drugs or who have HIV infection), cellular immunity is overwhelmed or fails to develop and progressive dissemination occurs. 411 Acute infection in the normal host, although common, is usually asymptomatic. Most cases of symptomatic histoplasmosis occur in patients with either a structural defect in the lungs, such as emphysema, 412 or some immunologic defect, which may or may not be definable. 413
The definitive diagnosis of histoplasmosis depends on growing the organism from infected sites or demonstrating it histologically in biopsy material. However, culturing H. capsulatum is difficult but, more important, it takes time. In disseminated disease the bone marrow is the best source for histologic identification of H. capsulatum; in one series the bone marrow examination yielded the organism in 15/19 cases. 414 Detection of H. capsulatum on bronchoalveolar lavage is useful in patients with acute or disseminated disease in whom there is evident pulmonary disease. 415
The widespread development of skin hypersensitivity to histoplasmin is taken as evidence that millions of people in endemic areas become infected with the fungus. More than 80% of individuals from highly endemic areas demonstrate skin test reactivity by their early twenties. 418 There is usually no definable clinical illness, but many adults in endemic areas show some radiographic evidence of infection, usually calcified foci of healed disease.
The chest radiograph findings (Fig. 5.98) of asymptomatic infection include the following:419. and 420.
Only gold members can continue reading. Log In or Register to continue