CASE 51 George Nomikos, Anthony G. Ryan, Peter L. Munk, and Mark Murphey A 45-year-old woman with rheumatoid arthritis was incidentally noted to have a lesion in the left fibular head. Figure 51A Figure 51B Figure 51C Figure 51D(See Figure 51D in color insert.) An anteroposterior radiograph of the knee (Fig. 51A) shows a vague area of radiolucency in the proximal fibular head with punctuate internal mineralization. There is no evidence of cortical destruction. A CT scan at the level of the fibular head (Fig. 51B) shows a well-defined lytic lesion with a narrow zone of transition. The lesion margin is partially sclerotic and partially nonsclerotic. There is internal matrix mineralization in a ring and arc pattern, compatible with a hyaline cartilage lesion. The lesion is predominantly very high signal intensity on the sagittal fat-suppressed T2-weighted image (Fig. 51C), similar to the signal intensity of fluid. The areas of low signal intensity on the T2-weighted image correspond to areas of mineralization on radiography and CT, and the lesion shows lobulated margins. Corresponding sagittally sectioned gross specimen of the fibular head (Fig. 51D) shows the glistening blue-white lobular lesion in the medullary canal. There is no evidence of destruction of the overlying cortex. Enchondroma. Enchondromas account for ~20% of all chondroid lesions of bone, are second in prevalence to osteochondromas (30%), and are the most common tumor of the hands. Lesions in the small bones of the hand account for ~40 to 65% of lesions and most commonly affect the proximal phalanges (40 to 50%) or metacarpals (15 to 30%). Long tubular bone lesions account for ~25% of enchondromas, and most commonly involve the femur, humerus, and tibia. Isolated flat bone or carpal bone involvement is very uncommon, and the possibility of chondrosarcoma should be excluded in the case of lesions in this location. Lesions arise when a fragment of hyaline cartilage from the growth plate becomes entrapped in the medullary canal metaphysis of a growing long bone. Instead of becoming ossified, it continues to grow and enlarge until skeletal maturity. As growth of the bone proceeds, the lesion may migrate into the diaphysis, which is more likely the earlier the lesion develops. Lesions are frequently discovered incidentally in asymptomatic patients in the third to fourth decades of life. Enchondromas also often present because of pathologic fracture, particularly in the case of hand lesions. Hand lesions may also cause mild surrounding soft-tissue swelling. Pain that is directly referable to a long bone enchondroma is worrisome for malignant transformation to chondrosarcoma (see Table 51–1).
Enchondroma
Clinical Presentation

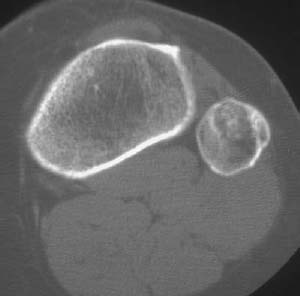
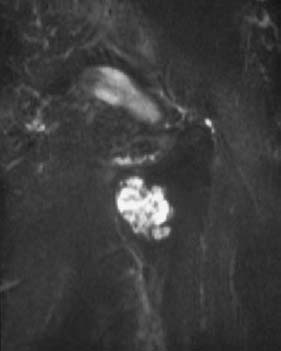

Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Clinical Findings
| Cortical scalloping > two thirds of the cortical depth in any one location |
| Uptake on scintigraphy greater than that seen in the anterior superior iliac spine |
| Cortical destruction |
| Soft-tissue mass |
| Pain directly referable to the lesion |
| Size > 5 to 6 cm |
| Epiphyseal location |
| Periosteal reaction or cortical thickening on radiography |
Pathology
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


