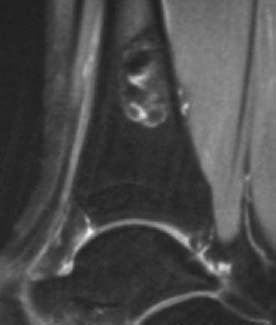
CASE 54 George Nomikos, Anthony G. Ryan, Peter L. Munk, and Mark Murphey A 15-year-old girl presented with ankle pain. Figure 54A Figure 54B Figure 54C Figure 54E The oblique radiograph of the ankle (Fig. 54A) shows an expansile lytic lesion centered in the cortex of the distal tibia. The lesion has a narrow zone of transition and a sclerotic rim. There is no aggressive-appearing periosteal reaction. The lesion is predominantly low signal intensity on T1-weighted images (Figs. 54B, 54C) but demonstrates a central area of high signal intensity that represents a residual island of normal fatty marrow entrapped in the lesion. The lesion is predominantly low signal intensity on the fat-saturated T2-weighted image (Figs. 54D, 54E) but does contain small regions of high signal intensity. Fibroxanthoma (nonossifying fibroma/fibrous cortical defect). The terms fibrous cortical defect, nonossifying fibroma, and fibroxanthoma are often used interchangeably to describe a related group of benign fibrous lesions of bone. The term fibrous cortical defect is best reserved for small lesions isolated to the cortical bone that commonly resolve spontaneously. The term nonossifying fibroma
Nonossifying Fibroma
Clinical Presentation

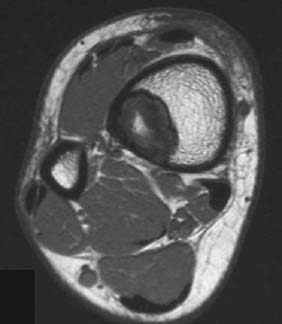

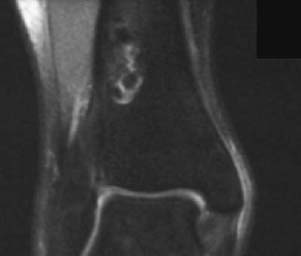
Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


