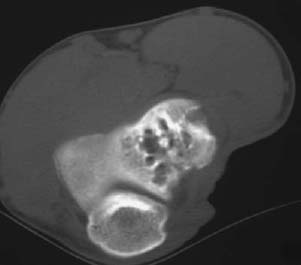
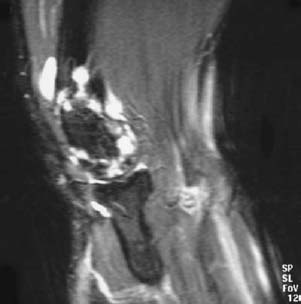
CASE 61 George Nomikos, Anthony G. Ryan, Peter L. Munk, and Mark Murphey A 28-year-old woman presented with elbow pain. Figure 61A Figure 61B Figure 61C Figure 61D An anteroposterior radiograph of the elbow (Fig. 61A) shows multiple round lucencies in the lateral humeral condyle with intervening trabeculae (reticular pattern). There is associated sclerosis around the areas of lucency. There is no associated periosteal reaction. The CT (Fig. 61B) demonstrates similar findings. The lucencies have a tubular appearance. No mineralized matrix is identified. Sagittal T2-weighted (Fig. 61C) and coronal inversion recovery (Fig. 61D) images show multiple high signal intensity tubular structures in the lateral humeral condyle extending into the surrounding soft tissues and into the elbow joint. The entire lesion is composed of these serpentine tubular structures. Osseous hemangioma. Angiomatous lesions, particularly hemangiomas, are very common in the musculoskeletal system. Although capillary hemangiomas are the most common type in general, they are usually very superficial, usually involute by age 7, and thus rarely come to radiographic evaluation. Cavernous hemangiomas, which are composed of large blood-filled vascular channels, are the form most commonly encountered by radiologists, as they usually involve the deep tissues and do not usually involute with age. Arteriovenous hemangiomas represent a localized abnormal persistence of a portion of the fetal capillary circulation and may be superficial (frequently asymptomatic) or deep (frequently symptomatic). They are almost exclusively soft-tissue lesions found in young patients and may cause complications associated with shunt vascularity. Venous hemangiomas are most commonly seen in the deep soft tissues of the retroperitoneum, mesentery, or lower extremity muscles and are composed of thick-walled vessels. Osseous hemangiomas are most commonly encountered in the vertebrae (thoracic or lumbar segments usually) or skull, accounting for 23% and 20% of all skeletal hemangiomas, respectively. Lesions in the vertebrae and skull are usually asymptomatic. In the vertebrae, hemangiomas usually originate in the vertebral body, but they may extend to involve the posterior elements or surrounding soft tissues, potentially causing neurologic compromise. Pathologic fracture may occur, but it is unlikely in lesions demonstrating significant trabecular thickening and reinforcement. Lesions that contain greater amounts of fat tend to be asymptomatic (quiescent hemangioma). Unlike spinal and skull hemangiomas, extremity lesions are symptomatic in > 90% of cases (pain, swelling, or mass). Appendicular lesions most commonly occur in the lower extremities (73%), particularly the tibia and femur. These lesions are most commonly medullary and are diaphyseal or metadiaphyseal, although periosteal and intracortical lesions also occur.
Osseus Hemangioma
Clinical Presentation


Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Clinical Findings
Imaging Findings
RADIOGRAPHY
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


