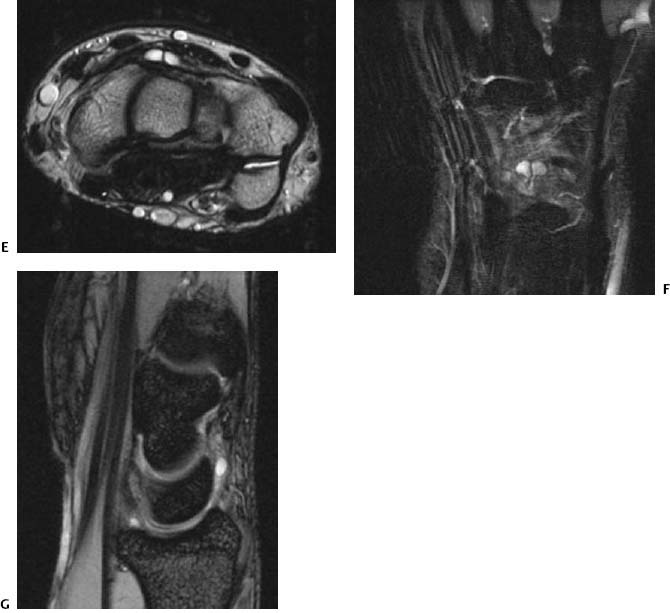
CASE 62 Anthony G. Ryan and Peter L. Munk A 29-year-old male snowboarder presented with an intermittent mass that “came and went” over a period of years, but that recently grew bigger and did not subside as usual. On examination, a large, minimally indentable firm swelling was palpable on the volar aspect of the wrist. The request read “suspected sarcoma.” Figures 62A Figures 62B Figures 62C Figures 62D MRI examination of the wrist shows a large lobular septated lesion palmar to the distal radioulnar joint that returns low signal intensity on a transaxial T1-weighted image (Fig. 62A) and high signal intensity on a transaxial T2-weighted image (Fig. 62B) and a coronal T2-weighted image with fat saturation (Fig. 62C). Within the scaphoid is a further lesion demonstrating similar signal characteristics and which, on the sagittal MPGR image (Fig. 62D), appears to be in continuity with the larger lesion. Normal signal intensity is returned from the remainder of the scaphoid. Large soft-tissue ganglion in contiguity with a small intraosseous ganglion of the scaphoid. None. The most common tumor of the soft parts of the hand, soft-tissue ganglia are mucin-containing unior multilocular cysts lined by flat, spindle-shaped cells arising from a tendon sheath, a joint capsule, a bursa, or a subchondral bone. The term synovial cyst is used synonymously when the lesion arises from a herniated joint capsule with synovium in contiguity. Although some sources distinguish these lesions (ganglia and synovial cysts) on this basis, the imaging literature at large does not, and all lesions in this chapter are referred to as ganglia. Ganglia are most frequently found in relation to the hand, wrist (Figs. 62E–62G), or foot (Figs. 62H–62K). An intraosseous ganglion is histologically identical to a soft-tissue ganglion but much less common, occurring in subchondral bone. Recognized as a potential source of mild pain, it occurs most frequently in the medial malleolus of the tibia, proximal tibia, femoral head, and acetabulum. Intraosseous ganglia have been described within the carpus and metacarpals. Of those occurring in the wrist, a scapholunate ganglion is relatively common, thought to be related to a tear of the dorsal scapholunate ligament. Both soft-tissue and intraosseous ganglia occur secondary to myxomatous degeneration of periarticular or intraosseous connective tissue, which is thought to happen as a result of repetitive trauma, possibly involving an ischemic element. It is thought that, as a result of trauma, a focal defect in a joint capsule or ligament, combined with subsequent myxoid degeneration, gives rise to a synovial herniation. The latter theory is supported by studies demonstrating a significant association of ganglia with internal derangements of the wrist, where between 28 and 45% of ganglia are associated with tears of the triangular fibrocartilage complex, the scapholunate ligament, or the lunotriquetral ligament. Figures 62E–62G Transaxial T2-weighted (62E), coronal STIR (62F), and sagittal MPGR (62G) images of the wrist show a very small bilobar ganglion arising from the dorsum of the carpus, which, despite its size, had been a cause of considerable discomfort for years. Subsequent arthrography (not shown) revealed a subtle tear of the dorsal scapholunate ligament. In the case of intraosseous ganglia, rather than an intrinsic osseous abnormality, it is thought that some arise secondary to erosion and penetration by an overlying soft-tissue ganglion, which may have been the etiology of the reference case (Figs. 62A–62D). This is not always the case, however, as intraosseous ganglia occur in the absence of associated soft-tissue ganglia. When the fluid within the ganglion becomes tense, the lesion acts as a mass and can consequently give rise to considerable discomfort due to pressure effects on adjacent nerves or vessels. The mass may interfere with joint excursion and, as a result, interfere with a patient’s occupation.
Ganglion
Clinical Presentation
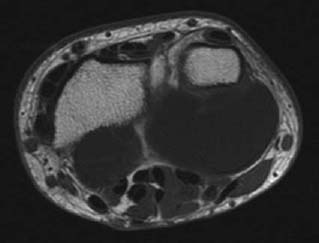
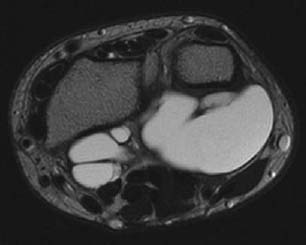
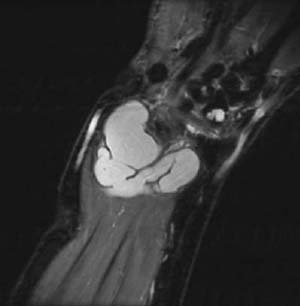
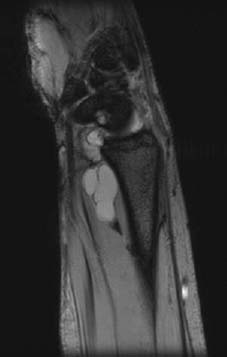
Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Etiology
Pathophysiology
Clinical Findings
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


