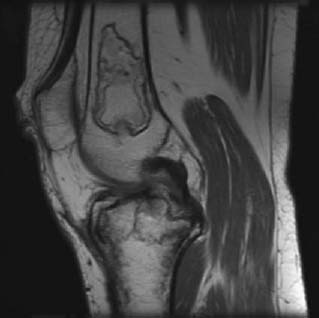
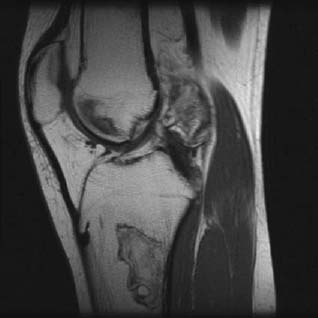
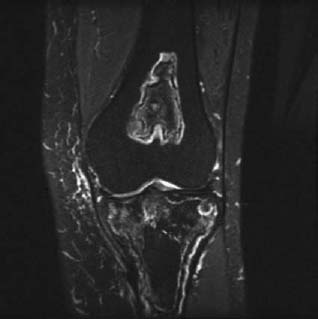
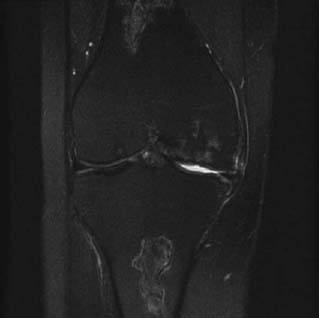
CASE 78 Hema N. Choudur, Anthony G. Ryan, Peter L. Munk A patient with systemic lupus erythematosus (SLE) presented complaining of right knee pain. An MRI was performed to exclude an internal derangement of the knee. Figure 78A Figure 78B Figure 78C Figure 78D A well-defined oval area of altered signal intensity is shown in the distal femoral diametaphysis that is isointense to bone on T1-weighted images with a hypointense serpiginous rim (Figs. 78A, 78B, T1 sagittal); hypointense on T2-weighted, fat-saturated images with a bright, hyperintense rim; and heterogeneously hyperintense on STIR sequences (78C, 78D, coronal STIR). Medullary bone infarct. There are two types of bone infarcts. The first involves only the diametaphyseal medulla with loss of the trabecular pattern and is usually clinically silent. The second involves the epiphyseal cortex and medulla, is usually subchondral and painful, and is often referred to as osteonecrosis or avascular necrosis, characteristically involving the femoral and humeral heads. Due to loss of blood supply, there is ischemic death of the marrow cellular elements. The extent and location of the lesion varies. It usually occurs in the long bones, frequently in the humeral and femoral shafts. Before the advent of MRI, bone marrow infarction was diagnosed with the use of conventional radiography and bone marrow scanning. Conventional radiographs show no acute changes, and areas of marrow ischemia are present only on follow-up examinations. Scintigraphic studies may not allow differentiation of acute from chronic marrow infarction. On MRI, acute marrow infarcts are often seen as focal marrow abnormalities. Focal marrow ischemia may arise secondary to intrinsic or extrinsic compression of the blood vessels or a combination of both. In the red marrow, cell death occurs in ~12 hours following anoxia, in the fatty marrow, it occurs within 5 days. The causative anoxia may be idiopathic, but trauma, dysbaric osteonecrosis, SLE, rheumatoid arthritis, scleroderma and collagen vascular diseases, sickle cell and other hemoglobinopathies, hemophilia, Gaucher’s disease, infection, pancreatitis, steroid intake, and diabetes are among the other causes. Of patients undergoing radiation therapy for breast cancer, 1 to 3% develop bone infarcts in the shoulder girdle. Hyperlipidemias are found to be associated with osteonecrosis in 80% ofpatients. The lesions may be unilateral, as in trauma or infection, or bilateral, as in caisson disease. In SLE, as in our case, the most commonly affected sites are the humeral head, femoral condyles, tibial plateaus, and talus. An unusual feature is the involvement of small bones of the wrist, hands, and feet.
Medullary Bone Infarct
Clinical Presentation
Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Etiology
Pathophysiology
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


