
Subacute Combined Degeneration with Optic Tract Involvement
Primary Diagnosis
Subacute combined degeneration with optic tract involvement
Differential Diagnoses
Copper deficiency
N2O overdose
Vacuolar myelopathy in AIDS
Vasculitis
Imaging Findings
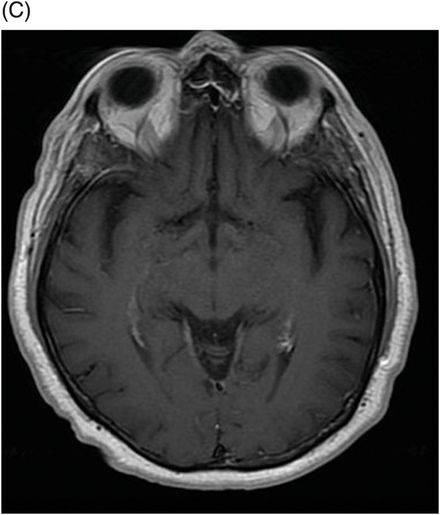
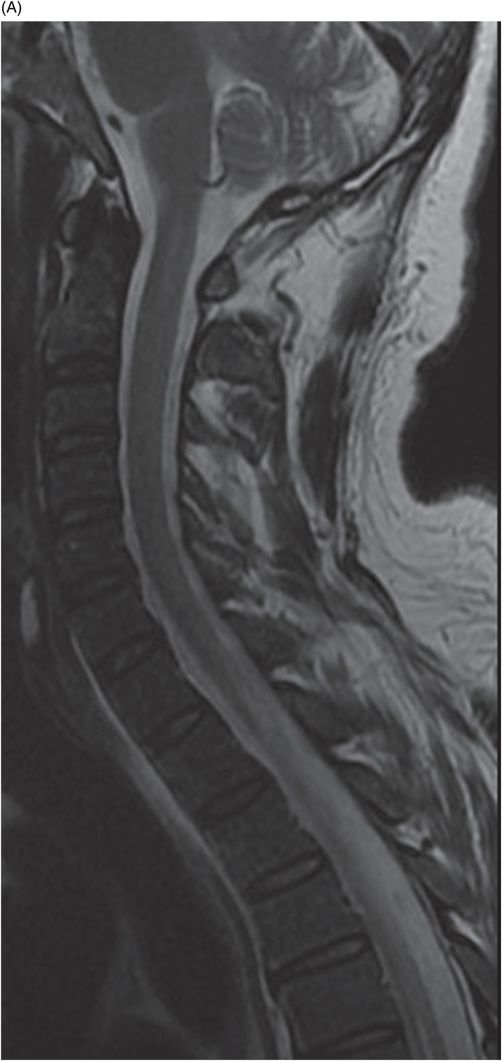
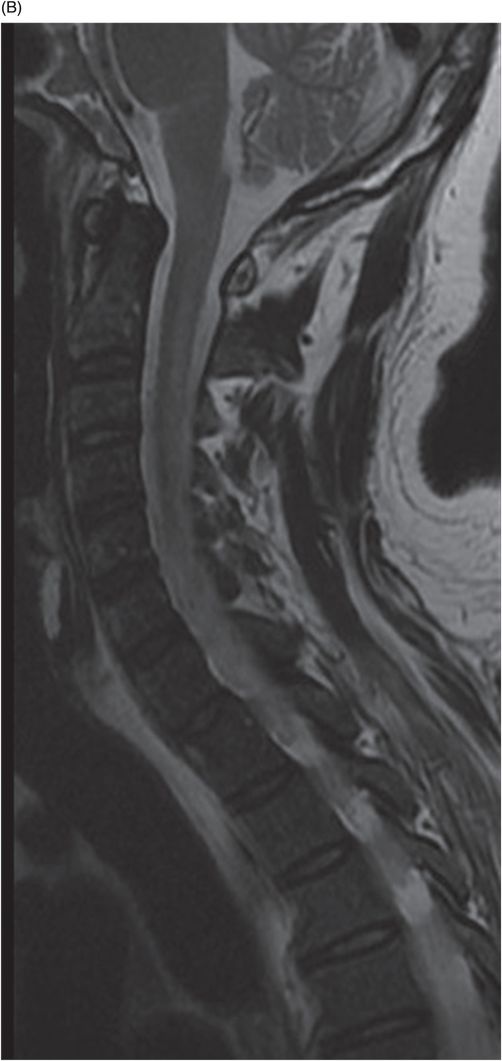
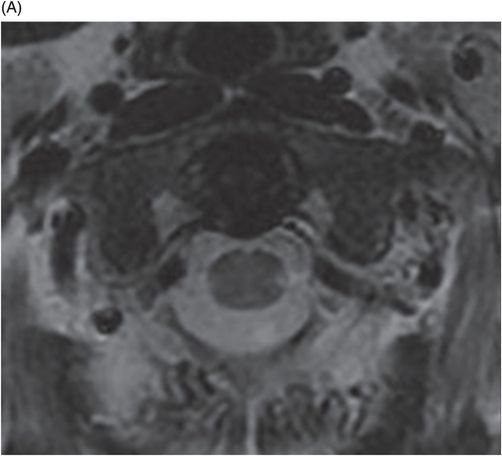
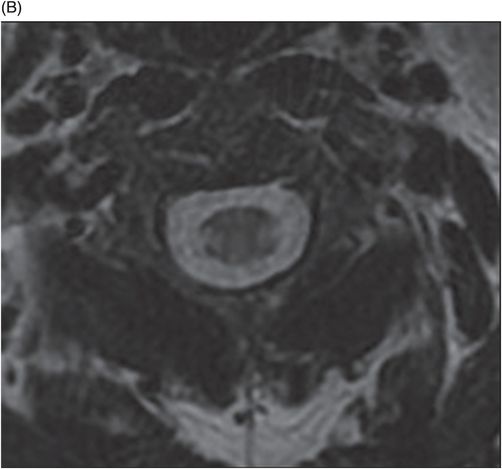
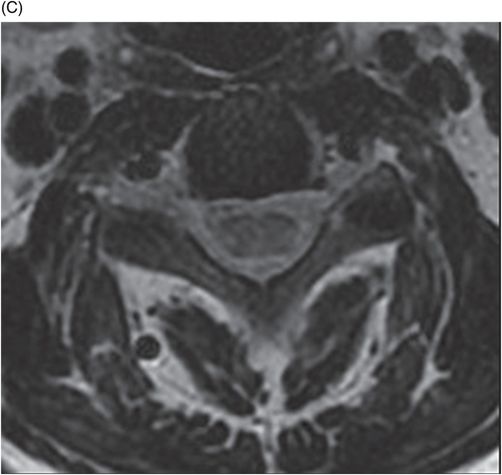
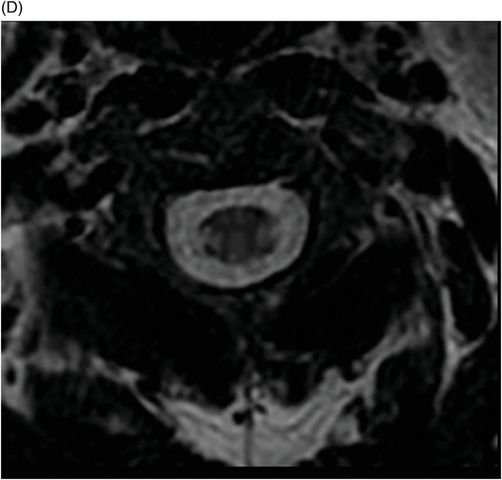
Fig. 79.1: (A) Axial FLAIR, (B) Axial T2WI, and (C) Postgadolinium axial T1WI demonstrated hyperintensity signal of both optic tracts without enhancement after contrast. Fig. 79.2: (A–B) Sagittal T2WI of the cervical spine showed a hyperintense signal in the lateral portion of the cervical spinal cord. Fig. 79.3: (A–D) Axial T2WI of the cervical spine showed hyperintensity signal of the dorsal and lateral columns of the spinal cord.
Discussion
Typical clinical presentation combined with typical imaging findings is diagnostic of subacute combined degeneration with optic tract involvement (SCDC). However, copper deficiency and N2O intoxication have identical imaging findings. Copper deficiency is indistinguishable from SCDC, both clinically and on imaging. A high level of suspicion is necessary for accurate diagnosis. History of N2O exposure, when present, is a clue to the right diagnosis. Identical imaging findings are seen in AIDS patients and sometimes in patients with vasculitis, but the clinical profiles are different in these patients.
B vitamins act as cofactors in numerous catalytic reactions required for the synthesis and function of neurotransmitters and myelin. Thus, vitamin B12 deficiency may result in injury to the neural tissue. Ludwig Lichtheim described the disease in 1887, recognizing that the pathology of spinal cord disease was associated with pernicious anemia and is different from tabes dorsalis. Subacute combined degeneration (SCD) of the spinal cord is an uncommon cause of myelopathy, but is the most frequent clinical manifestation of vitamin B12 deficiency.
Vitamin B12 is contained in essentially all meat and dairy products and is absorbed by the terminal ileum mucosa bounded to intrinsic factor, which is secreted by gastric parietal cells. This condition is usually seen in strict vegetarians, malabsorption syndromes such as bacterial overgrowth of the small bowel, pernicious anemia, regional enteritis, tropical sprue, or surgical procedures such as gastric fundus or ileal resection. Once internalized, intrinsic factor is released and vitamin B12 is transferred to other transport proteins and transported to the portal circulation. The vitamin B12 is mainly taken up by hepatic cells where it is liberated from the transport protein and methylated to methylcobalamin in the cytoplasm. Methylcobalamin plays a key role in the synthesis of methionine, which is further metabolized, to S-adenosylmethionine. S-adenosylmethionine is required in the synthesis of myelin. In vitamin B12 deficiency, this abnormal myelination has predilection for the posterior cord. N2O oxidizes the vitamin B12, makes it inactive, and renders the same effects of vitamin B12 deficiency.
Initial symptoms are usually paresthesia in the extremities and usually progress to sensory loss, gait ataxia, and distal weakness. Without treatment, the disease may develop to ataxic paraplegia. Physical examination can demonstrate loss of vibratory and joint position sense, weakness, spasticity, hyperreflexia, and extensor plantar responses. Visual abnormalities are well documented in the setting of vitamin B12 deficiency. Laboratory exams may reveal in the early stage low levels of blood vitamin B12, elevated homocysteine levels, and macrocytic anemia in the evolution, but they are not reliable markers for B12 deficiency.
Pathologically, there is a demyelination involving the dorsal and lateral columns (hence, the name combined degeneration) symmetrically, predominantly in the lower cervical and upper thoracic region, with spread in the cranial and caudal directions. This process is seen as hyperintensity on the T2WI and involves the dorsal and lateral columns. On sagittal images, there is a vertically oriented segment of variable length at the posterior aspect of the spinal cord. On cross-section images, bilateral paired areas of T2 hyperintensity are seen as an inverted V or inverted rabbit ears in the expected anatomic location of the dorsal columns. Enhancement can be observed in some cases. Magnetic resonance imaging appearance of the visual pathways in the setting of vitamin B12 deficiency has not been well documented in the literature. Bilateral symmetric T2 hyperintensities involving the optic tracts as shown in this patient is likely due to vitamin B12 deficiency as these abnormalities reverse with treatment.
The definitive diagnosis of vitamin B12 deficiency is usually made by a low serum B12 level (< 170 pg/ml by radioimmunoassay), or if the B12 level is borderline, elevated levels of the metabolites homocysteine and methylmalonic acid.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


