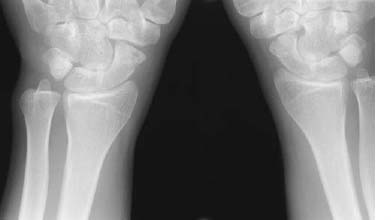
CASE 80 Peter L. Munk and Anthony G. Ryan A 30-year-old man presented with chronic wrist pain after a fall on his hand 24 months previously. Figure 80A An anteroposterior (AP) wrist radiograph (Fig. 80A) shows reduced joint space and osteophyte formation at the radioscaphoid articulation and an increased scapholunate interval. A dense triangular bony fragment is evident on the radial aspect of the lunate. Avascular necrosis of the proximal pole of the scaphoid with collapse. None. Scaphoid fractures represent approximately three quarters of all carpal bone fractures. This bone is critical to proper functioning of the wrist, and the morbidity of a poorly healed or unhealed fracture is significant. Although uncommon, fractures of the scaphoid in children tend to be avulsions of the distal pole, the latter accounting for 75%, with 20% of the waist and 5% of the proximal pole. The typical mechanism for a fracture is a fall on the outstretched hand. In adults, the most common site for a fracture is through the waist (Figs. 80B,80C), where ~70 to 75% occur. Twenty percent of fractures occur in the proximal third of the bone, with the remainder occurring in the distal portion (Fig. 80D), including the tuberosity (Figs. 80E, 80F). These fractures are often quite subtle, particularly as the fracture plane is transverse or slightly oblique. The blood supply of the scaphoid enters via the distal pole via dorsal and volar branches from the radial artery. Fractures through the waist or proximal portion therefore isolate the proximal pole from most of its blood supply, and it may become avascular. The more proximal a fracture, the more likely avascular necrosis is to occur. Figures 80B–80E An undisplaced fracture through the waist of the scaphoid. 80C A minimally displaced fracture of the waist of the scaphoid; a cortical step is evident on the radial aspect of the scaphoid. 80D A minimally displaced fracture of the proximal pole of the scaphoid; a cortical step is evident proximally at the scaphotrapezium articulation. 80E A minimally displaced fracture of the distal pole of the scaphoid through the base of the scaphoid tubercle, frequently seen best on a lateral view, as in this case. Figure 80F An AP radiograph of both wrists demonstrating bilateral scaphoid tubercle fractures. This is usually manifest as increased density of the proximal pole relative to the surrounding bones, which retain normal perfusion (Fig. 80A). Avascular necrosis may at times go on to heal if collapse does not occur.
Scaphoid Fractures
Clinical Presentation

Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Etiology
Pathophysiology

Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


