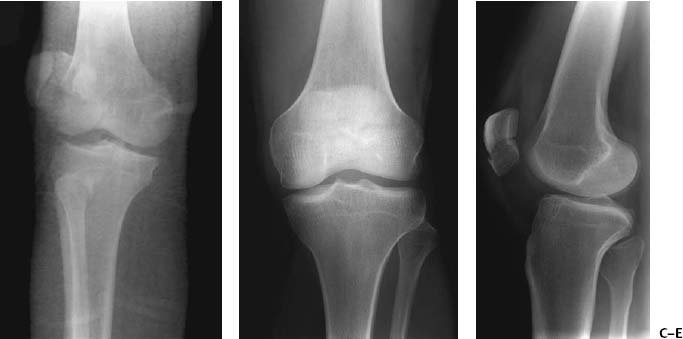
CASE 84 Hema N. Choudur, Anthony G. Ryan, and Peter L. Munk A young boy sustained an injury while playing soccer, after which he was unable to extend his knee. Painful swelling along the anterior aspect of the knee followed in the ensuing hours, with extreme tenderness overlying the patella. Figure 84A Figure 84B Anteroposterior (AP) and lateral radiographs of the knee (Figs. 84A, 84B) reveal a transverse distal third patellar fracture with no significant displacement of the fractured fragments. Transverse patellar fracture. Bipartite patella is usually seen at the superolateral edge of the patella and is unilateral in 57% and bilateral in the remainder, with a male:female predilection of 9:1. It is usually asymptomatic but may result in pain following a fracture or fibrous nonunion. On plain radiographs, the margins are smooth and corticated. Sinding-Larsen-Johansson disease, which is defined as osteochondrosis of the distal pole of the patella/tendinous junction, is related to chronic traction injury. This syndrome may mimic a stress fracture of the patella, an osteochondral sleeve fracture, or nonunited ossification center. It is well-differentiated on MRI, with high signal on inversion recovery sequences in the inferior aspect of the patellar tendon. Old healed injuries of the patella are seen on MRI as thickened patellar tendon. Insufficiency fractures of the patella are best differentiated on MRI with a low signal on all sequences. The patella is the largest sesamoid bone in the body and is present in the quadriceps tendon. The tendon includes contributions from the rectus femoris, vastus intermedius, medialis, and lateralis. It is anchored mainly to the tibial tuberosity. The medial retinacula attach the superomedial border of the patella to the medial tibial condyle, and the lateral retinacula, to the superolateral border and to the lateral condyle of the tibia. Overlying the patella is skin, subcutaneous fat, and the prepatellar bursa, making it a very superficial bone and consequently prone to direct injuries. It is lined posteriorly by articular cartilage. Usually, one ossification center is present, but this may vary up to three, seen between the ages of 2 to 6 years. Patellar fractures constitute 1% of all injuries. They may be transverse, vertical, marginal, or osteochondral (Figs. 84C to 84E). The diagnosis of each specific type is important as the management varies. Figures 84C-84E
Patellar Fracture
Clinical Presentation


Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


